Article Text

Abstract
Objective To find an association between metabolic non-communicable disease (NCD) risk factors (high blood pressure (BP), high random blood sugar (RBS) and overweight /obesity) and oral, breast, cervical cancers/precancerous or potentially malignant conditions.
Design This is an observational study using convenience sampling. The participants were screened through opportunistic or population-based screening.
Setting The study was conducted at a health promotion clinic (HPC) located in Northern India under the Indian Council of Medical Research. HPC is a screening clinic where screening is done for hypertension (HT), diabetes mellitus (DM), obesity, and oral, breast and cervical cancers. The study was conducted between December 2016 and January 2019.
Participant The number of participants screened was 8352 (6712 women and 1640 men). All consenting men and women above 18 years were included. All participants were screened for oral cancer, DM, HT and obesity. All women were also screened for breast and cervical cancers. Cervical screening was done for non-pregnant women 21 years and above with history of sexual activity.
Result Oral potentially malignant disease (OPMD) was the most prevalent, followed by breast cancer, oral cancer, cervical cancer and cervical precancer. High RBS had a strong association with oral cancer (OR=2.29, 95% CI 1.09 to 4.82, p=0.03) and breast cancer (OR=1.95, 95% CI 1.01 to 3.76, p=0.05). High BP had a strong association with breast cancer (OR=2.50, 95% CI 1.43 to 4.35, p<0.0001). An inverse association was noted between oral cancer and overweight/obesity (OR=0.20, 95% CI 0.08 to 0.48, p<0.0001). Current tobacco use was strongly associated with oral cancer (OR=6.51, 95% CI 3.63 to 11.67, p<0.0001) and OPMD (OR=9.82, 95% CI 8.13 to 11.86, p<0.0001). No association was elicited between the metabolic NCD risk factors and cervical cancer/precancer.
Conclusions The study reaffirms that NCD metabolic risk factors determine oral and breast cancers. Besides NCD risk factors, current tobacco use was a strong determinant of OPMD and oral cancer. Hence, primary and primordial prevention measures to control NCD metabolic risk factors and tobacco use should move along with secondary prevention of breast and oral cancers.
- Hypertension
- Diabetes Mellitus, Type 2
- oral cancer
- breast cancer
- Early Detection of Cancer
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Cancer is one of the non-communicable diseases (NCDs) in India whose incidence has risen from 1 million in 2012 to 1.5 million in 2018.1 Breast cancer, cervical cancer and oral cancer are the three most common cancers constituting 32.8% of all cancers among Indians.1 High blood pressure (BP), overweight or obesity and raised blood glucose are known metabolic risk factors for NCDs that are on the rise among Indians.2 With a rise in metabolic risk factors for NCDs, there may be a rise in cancer incidence. Population-based screening for hypertension (HT) and type 2 diabetes mellitus (DM) has begun in India since 2012. The government of India has launched the Operational Framework for Management of Common Cancers in 2016, and currently, it is in the early stages of rolling out the nationwide population-based screening of three common cancers, viz., oral, breast and cervical cancers.3 The National Institute of Cancer Prevention and Research (NICPR), under the Indian Council of Medical Research, has started a health promotion clinic (HPC) in February 2014 where screening for NCDs including cancer is being done.
Screening for cancers is a new concept for the Indian population. Hence, there are few studies from India that have tried to find an association between metabolic NCD risk factors and all the three cancers/precancerous or potentially malignant conditions. Hence, this study was undertaken to find if there is an association between them.
Methods
Study setting
The study was conducted at the HPC, NICPR, where screening is being done for HT, DM, obesity, oral cancer, cervical cancer and breast cancer. Both opportunistic and population-based screenings are being done at the HPC. Patients are referred to NICPR from nearby government, private and charitable health facilities for screening. In addition, patients who are referred to the NICPR for fine needle aspiration cytology (FNAC) clinic, along with their relatives, are motivated to get themselves screened. We regularly hold outreach awareness programmes in nearby villages, and individuals come to the clinic to get themselves screened. Most people availing the screening services hail from Gautam Buddha Nagar District of Noida or the nearby areas. For organised population-based cancer screening, seven nearby villages from the district were selected randomly. The Accredited Social Health Activist (ASHA) from these villages imparted knowledge and awareness regarding NCDs and cancer and the purpose and importance of screening. The ASHA motivates women and men to get themselves screened at HPC. A convenient sampling method was used for this study. All eligible men and women who came to the facility were imparted with knowledge and awareness regarding screening, and those who voluntarily gave their consent to undergo the tests were taken up in the study.
All men above 18 years were included in the study. They were screened for oral cancer, HT, DM and obesity. All women above 18 years were screened for HT, DM, obesity, breast cancer and oral cancer. Cervical cancer screening was done for sexually active women (present/past) above 21 years.4 Anyone aged less than 18 years and pregnant women were excluded from this study. Cervical cancer screening was not done for women aged less than 21 years, unmarried/single women with no history of sexual activity and women within the first 3 months of their postnatal period.
Operational definition
The operational definitions defined in the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke guidelines were followed for defining NCD metabolic risk factors, oral cancer, cervical cancer, cervical precancerous lesion and breast cancer5 (table 1). The definition given by the International Agency for Research on Cancer (IARC) for oral potentially malignant disease (OPMD) was followed.6 BG Prasad classification was followed for socioeconomic classification based on per capita income.7
Operational definitions
Data collection
A structured questionnaire was prepared covering sociodemographic details, general complaints, tobacco use history, gynaecological history, and breast and oral complaints. This questionnaire was pretested in an adjacent government health facility on 20 people. Data were collected on an online portal developed in the php format. Informed consent was obtained from every individual before being screened at this clinic for participating in this study and for undergoing the screening tests.
Data were collected through an interview with the study participants. The following physical measurements were done for all participants in the study: BP, height and weight, body mass index (BMI) and random blood sugar (RBS). Screening tests for oral, cervical and breast cancer screenings were also done for the study participants. Oral visual examination (OVE) was used for oral cancer screening, which was done by a trained dentist at the clinic. Further tests such as brush biopsy and/or biopsy from the abnormal area were done wherever applicable. Cervical cancer screening was done with Papanicolaou (Pap) smear test and visual inspection with acetic acid test. Women with abnormal tests were subjected to colposcopy and biopsy wherever applicable by an in-house trained gynaecologist. Clinical breast examination (CBE) was done for all women to screen for breast cancer. In case of abnormalities, ultrasound of the breasts, mammogram, FNAC and breast biopsy were done as indicated. The histopathological diagnosis was considered for the final diagnosis of breast cancer, cervical cancer and cervical precancer.
WHO STEPwise Approach to Surveillance recommendation was followed for physical measurements.8 BP was measured using the Omron (HEM-7200-AP3) digital blood pressure machine in the sitting position after 15 min of rest. The cuff was positioned on the right arm with the cubital fossa at the heart level. Three readings were taken at an interval of 2 min each. An average of the three readings was taken as the final reading.
A digital weighing machine (Omron HBF 212) was used to measure the weight of each subject. A portable stadiometer was used for measuring height. RBS was elicited by pricking the pulp of the index finger using a fresh lancet, and reading was noted using a glucometer and a glucose strip.5 Calibration of the anthropometric equipment was done routinely at weekly intervals. The Pap smear test, CBE and OVE were done as per the IARC recommendations.9 10
Data analysis
We exported the online data from php into an Excel sheet (V. 2016). Data were compiled and cleaned and further imported into SPSS software V.21 for analysis.
The categorical variables were analysed descriptively and the results were presented as proportions/percentages. Continuous variables were summarised using mean (±SD), and the difference in means was assessed using the independent sample t-test. To assess the association between the various cancers and precancers and the metabolic risk factors, univariate and multivariate logistic regression analyses were done. Crude/unadjusted and adjusted ORs were calculated, along with 95% CIs. A p value of ≤0.05 was considered to be statistically significant.
Results
Sociodemographic profile
In this study, we screened 8352 participants. Majority of them belonged to the 18–49 years age group (table 2). The average age of the study participants was 36.82 years. The mean age of women was 36.72 years and that of men was 37.26 years (table 3).
Sociodemographic profile of study participants
Descriptive statistics of continuous variables
Most of our participants were married Hindu rural women. Nearly half of our participants belonged to the middle class. One-third of the participants were illiterate (table 2).
Metabolic risk factors
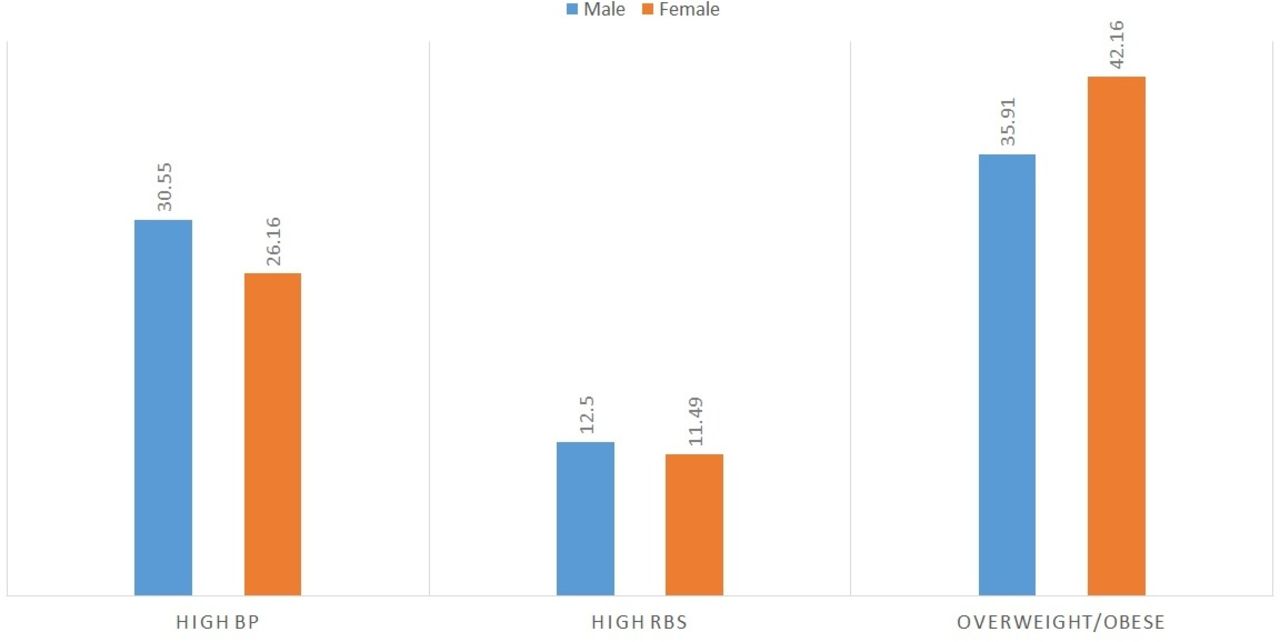
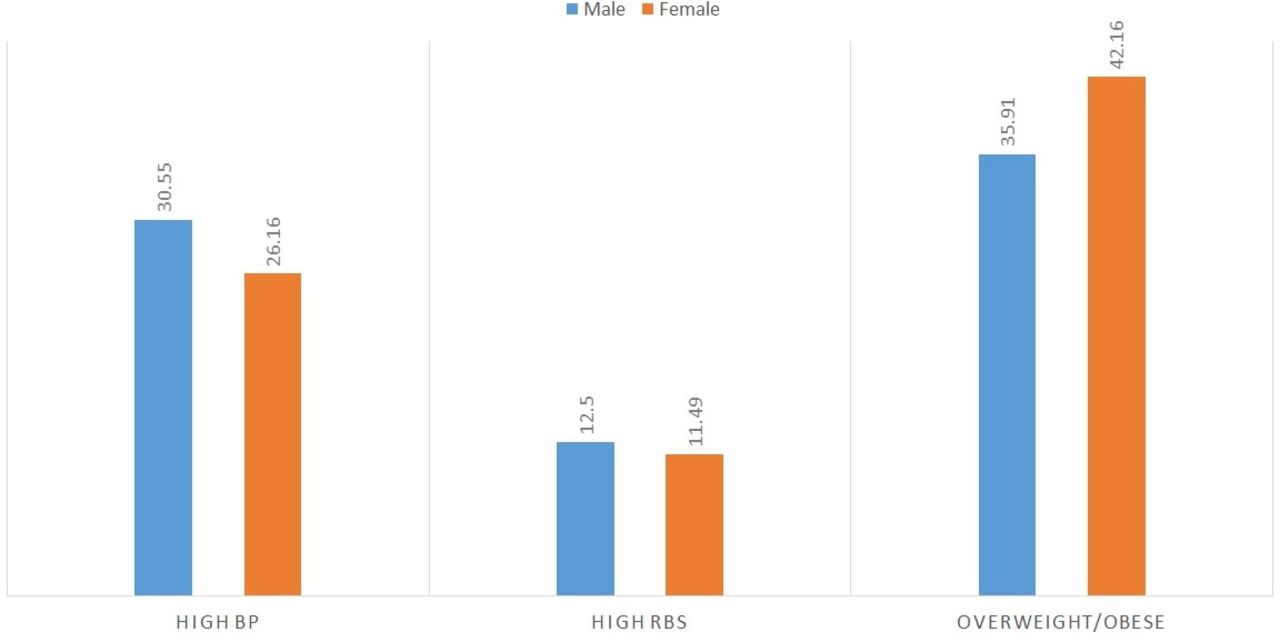
The prevalence of metabolic risk factors among study participants was as follows: 27.02% (2257/8352) had high BP, 11.70% (976/8352) had high RBS, and 40.94% (3419/8352) were overweight/obese. The prevalence of high BP was higher among men (30.52%) as compared with women (26.23%) (p<0.0001). Obesity was higher among women (42.21%) as compared with men (35.92%) (p<0.0001). (figure 1)
{kind=link}
Metabolic non-communicable disease risk factors among male and female participants. BP, blood pressure; RBS, random blood sugar.
The mean of continuous variables in the study are summarised in table 3. The mean systolic blood pressure (SBP) and diastolic blood pressure (DBP) of the male participants were significantly higher (p<0.0001 and p=0.01). The female participants showed higher BMIs than the male participants (p=0.01)
Prevalence of cancers and precancers
The prevalence of the three common cancers and precancers among the study participants is listed in table 4. Among the three cancers, breast cancer was most prevalent (0.63%) and cervical cancer was the least prevalent (0.51%). A significant number of individuals had OPMD (6.49%).
Prevalence of the three common cancers and precancers among study participants
As summarised in table 5, majority of patients with breast cancer were in the 30–49 years age group; those with oral cancer were in the 40 years and above age group; those with OPMD were in the 30–49 years age group, those with cervical cancer were in the 40 years and above age group; and those with cervical precancer were in the 30–39 years age group. The cervical cancer prevalence was similar in the 40–49 years, 50–59 years and 60 years and above age groups. Almost two-fifths of patients with breast cancer and two-thirds of patients with cervical cancer were postmenopausal. Majority of patients with oral cancer and OPMD were current/former tobacco users.
Descriptive measures for cancers and precancers
Association of metabolic risk factors with cancers and precancers
The association between metabolic risk factors and the three cancers or precancerous conditions is given in tables 6 and 7.
Characteristics of the metabolic risk factors in patients with cancers/precancers
Association between metabolic risk factors and cancers/precancers
Oral cancers and precancers
As summarised in table 7, high BP shows a strong association with OPMD in univariate analysis. However, as current tobacco use is a confounder in this association, on adjusting for the same, the association was found to be insignificant. No association was seen with oral cancer and high BP, and there was no association found in subgroup analyses among current and former tobacco users. High RBS shows strong association with oral cancer (OR=2.29, p=0.03) but no association was seen with OPMD.
Overweight and obesity were found to be negatively associated with oral cancer. This association was found to be strong after adjusting for current tobacco use (OR=0.20, p<0.0001). The association between lower BMI and oral cancer was found to be strong among the subgroup analyses of current tobacco users (OR=0.22, 95% CI 0.07 to 0.74, p=0.02), and the same was absent among the former tobacco users and never users.
Breast cancer
High BP was positively associated with breast cancer (OR=2.50, p<0.0001). This association was strongly positive among postmenopausal women (OR=3.24, p=0.02). High RBS was positively associated with breast cancer (OR=1.95, p=0.05). This association was also more among postmenopausal women (OR=3.05, p=0.01). No association was found between breast cancer and overweight and obesity. The association was also absent in subgroup analyses among premenopausal women and postmenopausal women.
In the stratified analysis among women above 45 years of age, the association between high RBS and breast cancer was found to be significant (OR=2.47, p=0.04). No significant association was found with high BP and overweight/obesity. No association was found between the metabolic risk factors and breast cancer in women aged below 45 years.
Cervical cancer and precancer
No association was found between metabolic risk factors and cervical cancer and cervical precancer.
Discussion
In the current study, high RBS had a strong association with oral cancer and breast cancer. High BP had a strong association with breast cancer. A strong inverse association was found between oral cancer and overweight/obesity.
The prevalence of high BP in our study population was 27.02%, which was consistent with the fourth District Level Household Survey, which reported HT in 25.3% of the study population (27.4% in men and 20% in women)11
The prevalence of high RBS in our study population was found to be 11.18%, which was a little more than the overall prevalence of diabetes (7.3%) elicited in the Indian Council of Medical Research (ICMR)–India Diabetes (INDIAB) study conducted in 15 states in India.12 The difference in the prevalence in the two studies may be due to a difference in the methodology. In the INDIAB study, fasting RBS followed by the oral glucose tolerance test was done, whereas in our study, only a single RBS value was considered.
The prevalence of overweight/obesity among our study population was 40.9%. In the ICMR–INDIAB study, the prevalence of obesity was found to be varied across different parts of India. The prevalence of generalised obesity was seen to range from 11.8% in Jharkhand to 31.3% in Chandigarh, which is located in Northern India.13 The higher prevalence in our study population may be due to the higher number of female participants. Many studies have shown that obesity was more among women as compared with men.14 15
Type 2 DM and obesity have been known risk factors for many cancers.16 17 The proposed mechanisms by which type 2 DM and obesity promote cancer development are hyperglycaemia, insulin resistance, hyperinsulinaemia, increased insulin-like growth factor levels, dyslipidaemia, inflammatory cytokines, increased leptin and decreased adiponectin.18
Breast cancer was the most common cancer among the study population, with a peak in the 40–49 years age group. Data from the population-based cancer registries (PBCRs) in India have also noted a peak in breast cancer between 45 and 49 years.19
A peak of oral cancer was seen in the 40–49 years age group in our study. However, the highest incidence rates of oral cancer in PBCRs in Northern India has been found in 60–69 years.20 The PBCR was based in Delhi and Punjab, and our data pertain to Noida, Uttar Pradesh. The variation between the two may be due to the regional variations in tobacco use. Delhi and Punjab have a lower prevalence of tobacco use, whereas a higher prevalence of tobacco use was seen in Uttar Pradesh as seen in Global Adults Tobacco Survey 2016–2017.21 As the present data are from a screening clinic where early detection of cancers and precancers is the main goal, the earlier presentation of oral cancers was seen in our study. A decreasing age of initiation of tobacco use may also be one of the reasons for presentation of oral cancer in the younger age group.
The highest prevalence of OPMDs was found among the 30–50 years age group. Leukoplakia, which is one of the common OPMDs, occurs in individuals aged 35–45 years.22 A hospital-based study in India found OPMDs to occur more commonly among individuals aged 21–30 years.23
Cervical cancer was found to be highest among the 51 years and above age group. This was also seen in the data gathered under the National Cancer Registry programme.24
High BP was found to be a strong determinant with an OR of 2.66 for developing breast cancer. A meta-analysis has demonstrated that women with HT have a relative risk (RR) of 1.15 to develop breast cancer as compared with other women with normal BP.25 The meta-analysis also showed that the positive association between breast cancer and HT was present for postmenopausal women, which was also seen among our study participants.
Overweight and obesity were not found to be significant risk factors for breast cancer, and this association was absent even on subgroup analyses based on menopausal status. However, dose–response meta-analyses of BMI and breast cancer risk showed that a higher BMI increased breast cancer risk among postmenopausal women, whereas a higher BMI could decrease breast cancer risk in premenopausal women.26
In this study, high RBS was associated with breast cancer (OR=1.95). A meta-analysis showed an increased risk of breast cancer in women with DM with an OR of 1.22.27 Another systematic review and meta-analysis showed that the overall HR for breast cancer incidence was 1.23 in patients with DM as compared with those without DM.28
A high RBS was also found to be a strong risk factor for oral cancer. A meta-analysis shows that individuals with type 2 DM have an RR of 1.15 to develop oral cancer in comparison with non-diabetic individuals.29 Our study also showed a positive association between type 2 DM and oral precancerous lesions (RR=1.85)
An inverse association was seen between overweight/obesity and oral cancer. This effect was seen among current tobacco users but was absent in participants who quit smoking or never smoked before. A population-based cohort study from the UK showed that underweight was associated with increased risk of oral cavity cancers, and this risk was driven by current smokers and past smokers.30 Other studies have also shown similar results.31 32 The differences in metabolic rates and different dietary patterns among smokers have been accepted as the mechanisms for this inverse relation between BMI and smoking.31 Current tobacco use was strongly associated with oral cancer (OR=6.51) and OPMD (OR=9.82) in our study. It is also supported by evidence from other studies.33–36
In the current study, no association was seen between cervical cancer and precancer and the risk factors under study. Conflicting evidence is present in the literature regarding the association of cervical cancer with the metabolic risk factors. Supportive evidence includes the ME-Can cohort study, which showed that elevated BMI, BP and triglyceride levels were associated with an increased risk of cervical cancer besides high glucose, which was a risk factor among women 70 years old and above37; a meta-analysis found a modest positive association of BMI with cervical cancer30; a prospective study from China found that there was an increased risk of persistent HPV infection and an increased risk of incident HPV infection among obese women; however, no association was found with hyperglycaemia or HT.38 Negative pieces of evidence are an observational prospective cohort study from China found significant decreased standardised incidence ratios for cervical cancer among patients with type 2 DM,39 and a prospective cohort study from Taiwan failed to show an increased risk of cervical cancer among hypertensive individuals.40
Strength and limitations of study
In the current study, data have been gathered from a large sample of population from a screening clinic. Because there are very few studies in literature from the India and Asia Pacific region on the topic, this study fulfilled the blank gap in this field and provided valuable evidence. The main limitations of this study are (1) the number of cancer and precancer participants were less; therefore all the associations with metabolic risk factors may not be evident; (2) the study population may not be representative of the true population as selection bias cannot be ruled out; (3) hyperlipidaemia is one of the NCD metabolic risk factors that was not included in the current study; and (4) few cases of breast cancer among women may not have been detected because CBE was a basic screening tool and its sensitivity is limited.
Conclusions
The current study brings forth the trends of the three most common cancers and their precursors in a population in India and their likely associations with metabolic NCD risk factors. As these NCD risk factors are increasing in numbers in India, we may expect the associated cancers to rise in the coming years. Hence, it becomes essential that besides early detection and management of cancers, the metabolic risk factors may be brought under control through primary and primordial preventive measures.
Key points
This study was conducted to explore and see if there is an association between oral, breast, cervical cancers and precancers with metabolic non-communicable disease risk factors, such as high blood pressure, high random blood sugar and overweight/obesity.
This study was conducted at a screening clinic in Northern India. An opportunistic and population based screening was done in this setting. A significant association was seen between high blood pressure and breast cancer. High RBS was associated with oral cancer and breast cancer. A low BMI was strongly associated with oral cancer. Besides other non-communicable disease risk factors, current tobacco use was also found to be strongly associated with oral cancer and OPMD. Cervical cancer and precancer were not found to be associated with any of the non- communicable disease risk factors.
Population based cancer screening is in it’s early stages in India. This study brings forth the trends of the three common cancers and precancers. The metabolic non-communicable diseases risk factors are on the rise in India. As few of these risk factors have been found to be associated with the cancers, we expect the population to be more at risk of developing these cancers if the non-communicable disease risk factors prevail among the population.
Acknowledgments
We acknowledge all the staff working at the health promotion clinic.
References
Footnotes
Contributors AK was responsible for data collection, data analysis, data interpretation, manuscript writing, original draft preparation and editing. RH was responsible for conceptualisation, methodology, writing, review, editing and supervision. VK was responsible for data compilation, data analysis, data interpretation and writing. KD was responsible for writing, review, editing and supervision. RM was responsible for conceptualisation, resources, funding acquisition, review, editing and approval of final manuscript.
Funding This study was funded by Indian Council of Medical Research.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval An ethical committee approval for this study has been given by the Institutional Ethical Committee (National Institute of Cancer Prevention and Research). The approval number is ICPO/IEC/2014.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.