Article Text

Abstract
Objective Predictors of prognosis are necessary for use in routine clinical practice for older patients with pneumonia, given the ageing of the population. Recently, the National Early Warning Score (NEWS), a comprehensive predictor of severity that consists solely of physiological indicators, has been proposed to predict the prognosis of pneumonia. The neutrophil/lymphocyte ratio (NLR) is a simple index of inflammation that may also be predictive of pneumonia. In the present study, we aimed to determine whether NEWS or a combination of NEWS and NLR predicts mortality in older patients with pneumonia.
Design A retrospective cohort study.
Setting A general hospital in Japan.
Participants We collected data from patients aged ≥65 years with pneumonia who were admitted between 2018 and 2020 (n=282; age=85.3 (7.9)). Data regarding vital signs, demographics and the length of hospital stay, in addition to the NEWS and NLR, were extracted from the participants’ electronic medical records.
Intervention The utility of the combination of NEWS and NLR was assessed using NEWS×NLR and NEWS+NLR.
Main outcome measures Their predictive ability for 30-day mortality as the primary outcome was assessed using receiver operating characteristic (ROC) curve analysis.
Results According to the NEWS classification, 80 (28.3%), 64 (22.7%) and 138 (48.9%) of the participants were at low, medium and high risk of mortality, respectively. The 30-day mortality for the entire cohort was 9.2% (n=26), and the mortality rate increased with the NEWS classification: low, 1.3%; medium, 7.8%; and high, 14.5%. The NLRs were 6.0 (4.2–9.8), 6.8 (4.8–10.4) and 14.6 (9.4–22.2), respectively (p<0.001). The areas under the ROC curves for 30-day mortality were 0.73 for the NEWS score, 0.84 for NEWS×NLR and 0.83 for NEWS+NLR, indicating that the combinations represent superior predictors of mortality to the NEWS alone. NEWS×NLR and NEWS+NLR tended to have better sensitivity, accuracy, positive predictive value and negative predictive value than NEWS alone (p=0.06).
Conclusions A combination of the NEWS and NLR (NEWS×NLR or NEWS+NLR) may be superior to the NEWS alone for the prediction of 30-day mortality in older patients with pneumonia. However, further validation of these combinations for use in the prediction of prognosis is required.
- Physicians, Primary Care
- Aging
- Clinical Medicine
- Community-Acquired Infections
- Community Medicine
Data availability statement
Data are available upon reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The National Early Warning Score (NEWS) has been reported to be a useful tool for the prediction of the prognosis of pneumonia in patients admitted to university and tertiary hospitals.
WHAT THIS STUDY ADDS
In the present study, we have shown that the NEWS is a predictor of 30-day mortality in older patients with pneumonia in a general hospital in Japan. Interestingly, we have also shown that the NEWS in combination with the neutrophil/lymphocyte ratio (NLR) (NEWS×NLR or NEWS+NLR) is superior in its prognostic ability to the NEWS alone.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The assessment of disease severity and risk stratification are essential to permit physicians to determine the appropriate location for a patient to be treated, whether as an outpatient, on a ward or in the intensive care unit. However, older patients may choose not to undergo aggressive treatment if they are close to death, even after a severity assessment. Instead, they may be transported to an institution that provides palliative care or be treated at home or in a nursing home. Thus, for the management of pneumonia in older patients, the NEWS and combinations of NEWS and NLR represent promising predictors of prognosis that can be rapidly calculated, not only in the emergency setting but also in the primary care and general medicine settings.
Introduction
In developed countries, including Japan, the population is ageing at an unprecedented rate, against the backdrop of a long-standing decline in birth rate. Pneumonia in older people is of increasing medical and economic importance.1 The management of pneumonia in such patients must involve an assessment of severity, to facilitate optimal care.2 Some popular scores (ie, the Pneumonia Severity Index and the Confusion, Urea, Respiratory rate, Blood pressure, 65 years score) are used for the assessment of community-acquired pneumonia (CAP), a common type of pneumonia.3 However, those popular CAP-associated scores are not always used by physicians in daily practice, primarily because of the large number of variables required to calculate each.4 5
The National Early Warning Score (NEWS) was designed as a standardised means of identifying acutely ill patients during hospitalisation.6 It consists of six physiological measures (respiratory status, requirement for supplemental oxygen, blood pressure, pulse rate, temperature and level of consciousness) that can be used to place patients into three risk categories (low, medium and high). For example, clinicians can use the NEWS to assess the need for the transfer of a patient from a general ward to the intensive care unit. Because the NEWS only includes physiological measures, it represents a simple and low-cost tool for the assessment of disease severity.
Previous studies regarding the use of the NEWS for the prediction of the prognosis of patients with pneumonia have generated conflicting findings regarding its superiority to other predictors. Studies of patients with CAP admitted to university and tertiary emergency hospitals have shown that the NEWS is superior,7 8 similarly useful9–11 or inferior12 to other predictors for use in patients with pneumonia. Interestingly, the addition of other predictors to the NEWS can improve its predictive ability. For example, a combination of the NEWS and the popular CAP-associated scores is better able to predict mortality than the NEWS alone.7 8 13 The NEWS-L, in which the circulating lactate concentration is added to the NEWS, was also found to be predictive of mortality in patients with pneumonia.12 In addition, because the leucocyte counts of patients are measured daily, the neutrophil/lymphocyte ratio (NLR), a simple and inexpensive marker of inflammation, has been recently proposed as a predictor of the prognosis of older patients with CAP14–17 or other types of pneumonia.18 However, the utility of a combination of NLR and the NEWS has not been assessed.
In previous studies of the prognostic value of the NEWS for patients with pneumonia, those admitted to university and tertiary hospitals have generally been recruited, and there have been no studies in the primary care or general medicine settings. In addition, despite the clinical importance of the management of CAP in older individuals, the previous studies were not specifically of older patients. Therefore, in the present study, we aimed to determine the utility of the NEWS alone and combinations of the NEWS and NLR, two simple indices, for the prediction of mortality in older patients with pneumonia who were admitted to a general hospital in Japan.
Methods
Study design and setting
We performed a retrospective study of the medical records of patients who were stated to have pneumonia at the time of admission.
Selection of study sample
Data were obtained for older patients (age ≥65 years) admitted to the General Medicine Department of our hospital between 1 April 2018 and 31 March 2020 who had been diagnosed with pneumonia. We identified the pneumonia to be CAP or nursing and healthcare-associated pneumonia.19 We diagnosed pneumonia comprehensively using respiratory symptoms (cough, sputum, dyspnoea and tachypnoea), other symptoms and signs (fever, tachycardia, anorexia, decreases of activities of daily living, impaired consciousness and incontinence), laboratory findings (markers of an inflammatory reaction, leucocytosis or leucopenia) and imaging findings (new or the worsening of pre-existing infiltrates on chest X-ray or CT).20 The diagnosis at admission was coded by the attending physician using this information. The participants were treated routinely, according to the recommendations of the major Japanese clinical guidelines,21 and we followed them until they were discharged from the hospital.
The exclusion criteria were as follows: (1) transfer from another hospital, discharge from the hospital within 10 days or a diagnosis of hospital-acquired pneumonia; (2) the presence of empyema, pulmonary tuberculosis, pulmonary oedema, pulmonary thromboembolism or non-infectious interstitial pneumonia; (3) previous administration of antibiotics by another physician; (4) immunosuppression, treatment with a corticosteroids, or chemotherapy within the preceding 90 days or radiotherapy; (5) the presence of liver disease or a haematological disorder that might affect the incidences of inflammation measured22; and (6) missing baseline data regarding any element of the NEWS or NLR.
For older patients with pneumonia, with an effect size of 0.25, an α level of 0.05 (5%), a β level of 0.20, a power of 80% and a two-sided analysis, the required sample size was calculated to be 53 per group. The power analysis was performed using G*Power V.3.1.7.9 for Windows (Franz Faul, University of Kiel, Germany).
Outcome measures
The primary outcome was 30-day mortality following a diagnosis of pneumonia and the secondary outcome was the length of hospital stay.
Data collection and processing
We collected demographic data, data regarding comorbidities and the laboratory findings at baseline. Specifically, the age, sex, body mass index (BMI), vital signs, comorbidities (dementia, cerebrovascular disease, congestive heart failure, chronic respiratory disease, chronic kidney disease and malignant disease), medication (for hypertension, diabetes mellitus and/or dyslipidaemia), Charlson comorbidity index,23 number of prescriptions, presence of polypharmacy (use of ≥5 medications), place of residence before admission and level of care of the participants were collected. The laboratory data collected were the serum albumin, urea nitrogen and C reactive protein (CRP) concentrations; the haemoglobin concentration; and the white cell, neutrophil and lymphocyte counts. These variables were used to calculate the NEWS and NLR. We treated these variables as potential confounders of the analysis of mortality owing to pneumonia in the older participants, as described in previous reports.7–13
The NEWS was calculated using data regarding six physiological parameters that were collected during hospitalisation: respiratory rate, oxygen saturation, body temperature, systolic blood pressure, pulse rate and the level of consciousness.6 Every continuous variable was awarded a maximum score of 3 points, whereas the need for supplemental oxygen and the level of consciousness were awarded 0 points if absent/normal and 2 or 3 points if present/altered. Participants with a NEWS of 0–4 points were classified as low risk, those with a NEWS of 5–6 points were classified as medium risk and those with a NEWS of 7+ points were classified as high risk. However, when a single physiological parameter received a score of 3 points, the participant was categorised as being at medium risk, instead of low risk. To rate any confusion, we reviewed the medical records of the participants at the time of admission and recorded the presence of any abnormalities in the Alertness, response to Voice, Pain, Unresponsiveness score, a Glasgow Coma Scale score of ≤13, abnormalities identified during the mental status examination, and any confusion or delirium.
Total leucocyte and leucocyte fraction counts were obtained by fluorescence flow cytometry and hydrodynamic focusing (forward and side scatter) using a Sysmex XT-2000i automated haematology analyser (Sysmex, Kobe, Japan) and peripheral blood diluted in EDTA. Platelet counts were performed using sheath flow direct-current detection, and the circulating CRP concentration was measured by immunoturbidimetry using a TBA-2000FR instrument (Canon Medical Systems, Tochigi, Japan). NLR was calculated using the results obtained during routine haematological analyses. The values for each of these markers of inflammation were compared among the NEWS categories.
Statistical analysis
The Kolmogorov-Smirnov test was used to analyse the normality of the collected datasets. Categorical datasets are presented as frequency (%), and continuous datasets are presented as mean (SD) for parametric data or median (IQR) for non-parametric data. The Χ2 test was used to compare the proportions for the categorical data. Analysis of variance and the Kruskal-Wallis test were used to analyse normally and non-normally distributed continuous datasets, respectively, among the three groups. Time-to-event data were evaluated using Kaplan-Meier estimates. A Cox proportional hazards model was used to perform a sensitivity analysis to ascertain whether the NEWS is a useful predictor, even after the exclusion of factors associated with pneumonia. Variables for which p<0.20 that were obtained during the univariate analysis of the baseline data were included in a multivariate-adjusted Cox proportional hazards analysis of 30-day mortality. The discriminability of each index for 30-day mortality was assessed using the area under the receiver operating characteristic curve (AUC) and 95% CI.24 The optimal cut-off value, sensitivity and specificity were determined using the Youden index,25 and differences in the AUC were identified using DeLong’s test.26 Positive (PPVs) and negative predictive values (NPVs) were calculated to assess the accuracy of the NEWS alone and the combinations of NEWS and NLR. To compare the sensitivity, specificity, accuracy, PPV and NPV, McNemar’s test was used.27 28 Statistical significance was defined as a two-sided p<0.05. Analyses were conducted using SPSS V.28 (IBM). We did not include participants with missing baseline data, and in particular those with missing laboratory data.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Participants
During the present study, 446 people of ≥65 years of age were diagnosed with pneumonia, of whom 164 were excluded (76 because of treatment with antibiotics, 17 because of corticosteroid use, 44 because of the presence of a haematological disease, 7 because of the presence of a liver disease and 20 because of missing data), leaving 282 for inclusion in the final analysis (online supplemental figure 1). Because all the participants were hospitalised, we were able to readily follow them until they were discharged.
Supplemental material
Characteristics of the cohort
Table 1 shows the baseline characteristics of the study sample (age=85.3 (7.9); 56.7% male), categorised according to the NEWS classification. The low NEWS group included five participants with 0 points. The 30-day mortality rate for the entire group of participants was 9.2% (n=26). With respect to the outcomes, both the 30-day and in-hospital mortality rates and the duration of the hospital stay significantly increased with the NEWS category. Figure 1 shows the Kaplan-Meier curves for the 30-day mortalities of the low, medium and high NEWS risk groups (log-rank test, p<0.03). Dementia was the most frequent comorbidity (65.2%), followed by cerebrovascular disease (34.8%) and congestive heart failure (21.6%). With the exception of sex, there were no significant demographic differences between the participants in each NEWS category. With the exception of systolic blood pressure, all the vital signs of the participants were significantly worse in the high NEWS group. There were no significant differences in the albumin, haemoglobin or urea nitrogen concentrations among the groups. The white cell count, neutrophil count and NLR were higher in the high NEWS group than in the other groups.
Baseline characteristics and outcomes of the participants, categorised according to the NEWS

Kaplan-Meier curves for 30-day mortality for the low, medium and high NEWS groups. NEWS, National Early Warning Score.
Relationships of the outcomes with potential predictor
Table 2 shows the results of the univariate and multivariate analyses of the relationships between 30-day mortality and parameters at baseline. On univariate analysis, there were parameters showing a significant relationship with 30-day mortality for age, BMI, chronic kidney disease, neoplastic disease, level of care, albumin, urea nitrogen and the NEWS. Then, NEWS and urea nitrogen were entered into the multivariate analysis. Because chronic kidney disease and neoplastic disease had less than 10 deaths, the variables were not used in the multivariate analysis to avoid the possibility of overfitting and the distortion of the model. Table 3 shows the HRs for 30-day mortality by the Cox proportional hazards model in the participants as categorised according to the NEWS category. We obtained a crude HR, an HR adjusted for age, and an HR adjusted for age and urea nitrogen, identified as risk parameters for mortality in table 2 versus the low NEWS group. The age-adjusted and multivariate-adjusted HRs for the high NEWS group were 8.87 (95% CI: 1.19 to 66.20, p=0.03) and 8.69 (95% CI: 1.17 to 64.81, p=0.04), indicating significant associations with high 30-day mortality.
Results of the univariate and multivariate Cox regression analyses performed to identify prognostic factors for 30-day mortality in older patients with pneumonia
HRs (95% CIs) for the 30-day mortality rates of the participants, categorised according to the NEWS
Evaluation of model performance
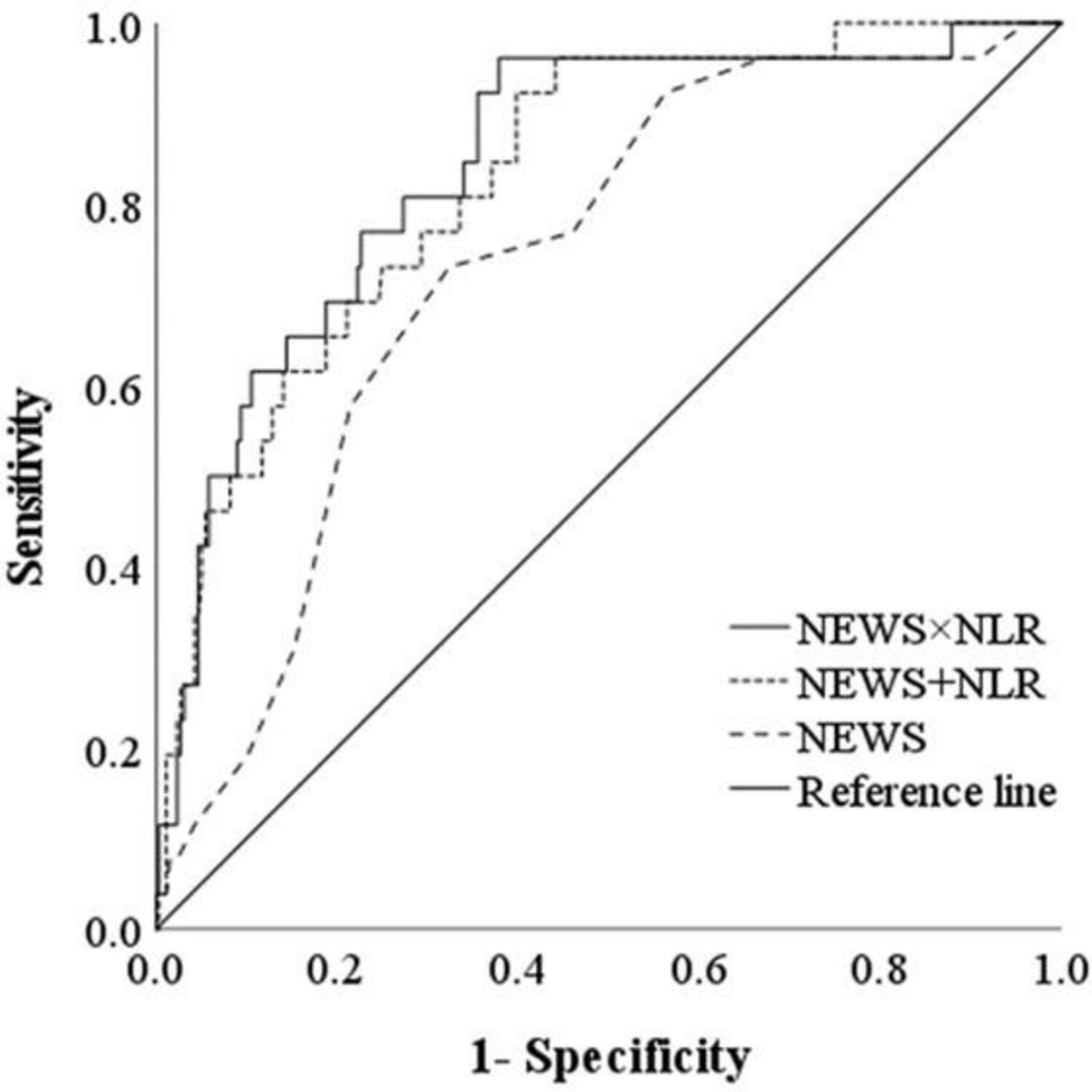
Figure 2 shows the predictive ability of the NEWS alone, NEWS×NLR and NEWS+NLR. The AUC analysis showed that the NEWS was a moderately good predictor, with an AUC of 0.73. The AUCs for NEWS×NLR and NEWS+NLR were 0.84 and 0.83, respectively, implying significantly better prognostic ability than the NEWS alone (p=0.007 and 0.04, respectively). The optimal cut-off values, sensitivities and specificities for the AUCs were 7.5, 73.1% and 67.6% for the NEWS alone; 65.1, 96.2% and 62.1% for NEWS×NLR; and 17.4, 92.3% and 60.2% for NEWS+NLR, respectively (table 4). The PPV, NPV and accuracy for each predictor of 30-day mortality, compared with NEWS alone, are also shown in table 4. NEWS×NLR and NEWS+NLR tended to have better sensitivity, accuracy, PPV and NPV than NEWS alone, but these differences were not statistically significant (p=0.06).

{kind=link}
{kind=link}
Receiver operating characteristic curves and the corresponding areas under the curves for the risk of 30-day mortality, according to the NEWS alone, NEWS×NLR and NEWS+NLR. NEWS, National Early Warning Score; NLR, neutrophil-to-lymphocyte ratio.
Areas under the receiver operating characteristic curves (AUCs) for the various predictors of 30-day mortality
Discussion
In the present study, we have shown that the NEWS is a predictor of 30-day mortality in older patients with pneumonia. Interestingly, we also found that the NEWS×NLR and NEWS+NLR combinations have superior prognostic ability to the NEWS alone. The ability to predict the prognosis of pneumonia in older patients using these simple and inexpensive markers should help facilitate the appropriate management of such patients in a primary care setting.
The NEWS was previously validated for use as a track-and-trigger system for acute illness.6 In the present study, we found a moderate discriminatory ability in the AUC for the NEWS (0.73). The optimal cut-off value for the NEWS for older patients with pneumonia was found to be 7 in the present study, consistent with previous reports recommending an emergency response and transfer to an intensive care unit if the NEWS score is higher than 7 points.6
Although the addition of the NLR to the NEWS increased its predictive ability, the explanation for this is not yet clear. In inflammatory conditions such as pneumonia, the neutrophil count increases because of delayed apoptosis and the stimulation of stem cells, whereas the lymphocyte count decreases because of greater apoptosis and the migration of these cells to the liver, spleen and lymphoreticular system. Together, these changes result in an increase in the NLR.29 Patients with severe infections experience more lymphocyte apoptosis than patients with sepsis but no shock, and this is associated with greater mortality.30 Therefore, the NEWS and NLR are overlapping means of assessing inflammatory conditions, and combinations of NEWS and NLR represent superior methods of identifying infection.
The assessment of disease severity and risk stratification are essential for physicians to determine the appropriate location for a patient to be treated, whether as an outpatient, on a ward or in the intensive care unit. However, older patients may choose not to undergo aggressive treatment if they are close to death, even after a severity assessment. Instead, they may be transported to an institution that provides palliative care, or be treated at home or in a nursing home. Thus, for the management of pneumonia in older patients, the NEWS and combinations of NEWS and NLR represent promising predictors of prognosis that can be rapidly evaluated, not only in the emergency setting but also in the primary care and general medicine settings.
The present study had several limitations. First, because it was a single-centre retrospective study of medical records, it lacked some external validity. Therefore, a prospective multicentre study should be conducted in the future to confirm the usefulness of the NEWS as a predictor of the prognosis of pneumonia in older patients. Second, we only studied inpatients, meaning that the number of patients with minor illnesses was low, which may have skewed the results. Third, the treatments used, such as antibiotics and oxygen therapy, were not included as a variable in the study, meaning that factors related to this choice may not have been accounted for in the analysis. Finally, the classification of pneumonia varies according to the environment in which a patient lives. However, in older patients, the actual type of pneumonia is often unclear. Therefore, the participants in the present study were representative of patients with pneumonia in general.
Conclusion
We have shown that the NEWS is a predictor of 30-day mortality in older patients with pneumonia, and also the superiority of combinations of the NEWS and NLR (NEWS×NLR and NEWS+NLR) to the NEWS score alone for the prediction of 30-day mortality in older patients with pneumonia. However, further studies should be performed to validate the use of these indices for the prediction of prognosis in such patients.
Data availability statement
Data are available upon reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
The Institutional Review Board approved the study (approval number: 2022-008; approval date: 9 June 2022). The requirement for written informed consent was waived because of the retrospective nature of the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors made substantial contributions to the acquisition, analysis and interpretation of the data. EK and KK conceived and designed the study. EK, RU, NO, YA, TO, SS, AH, TN, KS and SA collected the data. EK performed the statistical analysis. EK drafted the manuscript. KK critically reviewed and revised the manuscript. All authors read and approved the final version of the manuscript. EK is the guarantor of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.