Article Text

Abstract
Objective Women suffering from mental health problems require varied needs of mental health service utilisation. Transition between general practitioner and mental health services use are available through the Better Access Scheme initiative, for those in need of treatment. The study’s aim was to identify trajectories of mental health service utilisation by Australian women.
Design The Australian Longitudinal Study on Women’s Health data linked to the administrative medical claims dataset were used to identify subgroups of women profiled by their mental health service use from 2006 to 2013. Latent growth mixture model is a statistical method to profile subgroups of individuals based on their responses to a set of observed variables allowing for changes over time. Latent class groups were identified, and used to examine predisposing factors associated with patterns of mental health service use change over time.
Setting This study was conducted in Australia.
Participants National representative sample of women of born in 1973–1978, who were aged between 28 and 33 years at the start of our study period.
Results Six latent class trajectories of women’s mental health service use were identified over the period 2006–2013. Approximately, one-quarter of the sample were classified as the most recent users, while approximate equal proportions were identified as either early users, late/low user or late-high users. Additional, subgroups were defined as the consistent-reduced user and the late-high users, over time. Only 7.2% of the sample was classified as consistent high users who potentially used the services each year.
Conclusion These findings suggest that use of the Better Access Scheme mental health services through primary care was varied over time and may be tailored to each individual’s needs for the treatment of depressive symptoms.
- Depression
- Health Services
- Mental Health
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Uptake of the Australian Better Access Scheme subsidised mental health services has been well received, though some social, economic and geographical inequities are evident. However, service use over time using large scale studies have not yet been evaluated.
WHAT THIS STUDY ADDS
This research finds that over the 7-year study period different trajectories of service use by women were identified providing valuable insights on varied use of the government subsidised mental health services in Australia.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
The study identified different trajectories of mental health service use and highlights the need for flexible and individual tailoring of health services, especially mental health services.
Introduction
In 2006, the Australian federal government allocated funding to facilitate access to mental health services by initiating new subsidies through the Medical Benefits Scheme (MBS) specifically for mental health services. Under the Better Access Scheme (BAS) a range of new general practitioner (GP), psychology, selected social worker and occupational therapy services were made available for those people with diagnosed mental health problems.1 Despite efforts to implement the BAS as a universally subsidised service, equity of access to mental healthcare services has not always been achieved.2–4
For most people experiencing from some form of psychological distress, accessing services is critical in achieving improved mental health.5 6 The patient’s perceived need for services has been found to play an important role in accessing care. People identified counselling services as a facility for gaining an understanding of their illness, recognising stressors such as relationship difficulties, and for determining when to move away from a sole reliance on medications.7 However, Meadows and Bobevski8 found that while most people using mental health services in Australia consult a GP, psychiatrist or a psychologist they also noted that a significant proportion of participants reported an unmet need, and those who received care were often unclear as to whether sufficient help was received.
Unmet needs can be due to a number of barriers, of which financial cost9 10 and concern for social discrimination are the most significant.11–13 Satisfaction with mental healthcare was seen by patients as achievable when sufficient support and assistance were received and those reporting satisfactory care generally had improved mental health.7 14 Dissatisfaction with treatment was also found to be attributable to a number of factors (such as caregiver assistance, inadequate and poor treatment) generally leading to more difficult lives for people suffering with mental health problems.15
People suffering from depression or anxiety experience disproportionately higher rates of disability and mortality compared with the general population.3 16 17 Therefore, mental health services need to provide a treatment path to recovery through an integrated approach with continuity of care suited to each individual.18 19 Ideally, if policy and resource priorities are to be effectively identified, the individual’s perspective is necessary in order to understand the need for mental healthcare, who seeks help and the type of help required to improve mental health. To date, modifications to strategies aimed at satisfying the policy of national access equity requires an understanding of the attributes of those who do and do not use the BAS services, and an understanding of the impediments impacting service access.20
Under the BAS an initial, referral by a GP to five counselling sessions are provided with a further five available following a GP review per calendar year. An additional five sessions are available in exceptional circumstances only. Services are not expected to be ongoing or to be provided over multiple years,1 however, where patients are in need of mental health services they may access up to 15 per year. Many studies evaluating the BAS initiative21 22 have generally found that the scheme has contributed to the improvement of consumer health. However, others2 22 23 claim a methodological weakness in these BAS evaluations, stating that evidential evidence could not be provided on the effectiveness of the initiative.
Numerous studies have examined the introduction of the BAS and the characteristics and determinates of use of the mental health services.2 21 24–28 Many studies have found that the BAS is providing access to care for those with psychological distress but gaps in the literature exist on service delivery of inequitable access to good quality healthcare for those with the greatest need. Despite efforts to implement the BAS as a universally subsidised service, equity or access to mental healthcare services has not always been achieved.2 29 30 Additionally, service demand for mental healthcare has been shown to vary among Australian adults and treatment patterns follow a gradient based on need.29–31 Yet, while these studies show evidence of service use and need, no study to date has assessed use of the mental health services over time.
Little is known about the intersection of mental health service use among the subpopulations of women who are high risk of need, let alone the complexity of their mental health service use. Therefore, the aims of this study are to examine patterns of mental health service use over time among high-risk women that have a mental health plan under the BAS and to examine the associations between use of BAS mental health services and demographic covariates. To address the study’s goals, we hypothesised those Australian women who have a need for mental health services will access the government’s subsidised services for the recommended number of government allocated visits per year, and that only a subgroup of women will not access the mental health services. We aim to (1) determine the proportion of women that have a GP mental health assessment but do not use the allocated mental health services; (2) identify subgroups of women who show similar patterns of mental health service use over time and (3) examine the characteristics that define women into each subgroup. Further, we expect to determine the characteristics of, barriers to and specific use of BAS mental health services by the defined subgroups of women.
Methods
Participants
Data were provided by the Australian Longitudinal Study on Women’s Health (ALSWH), which is a longitudinal cohort study on women’s health, well-being and lifestyle.32 33 The study began in 1996 and consisted of a random sample of over 40 000 women across three age cohorts, the 1973–1978, 1946–1951 and the 1921–1926 birth cohorts. The study’s first data were collected in 1996 and women have been surveyed on a routine basis every 3 years, to-date the study has collected up to seven surveys of information. In 2013, the ALSWH study recruited a further 17 000 women from a fourth cohort, the 1989–1995 who have been surveyed annually. The study sample for this research consisted of all women from the ALSWH who participate in the 1973–1978 Cohort34 who were aged between 28 and 33 years at the start of our study period and due to the higher proportion of women from the 1973 to 1978 cohort having used the BAS services,35 women from the 1989 to 1995 cohort had not yet been collected and were not eligible for the study period Women consented to survey data33 are routinely linked to data from the MBS which is Australia’s universal health insurance scheme. These data provide information on dates of visits to GPs (unreferred visits), medical specialists (referred visits), diagnostic and procedural tests, health assessments and all allied health service use. To be eligible for this study, women had to have claimed at least one of the subsidised Medicare items under the BAS: initial GP consultation any psychological therapy services, focused psychology strategies or GP mental health treatment (online supplemental S1)1 between 1 January 2007 and 31 December 2013. Of the 14 247 women from the 1973 to 1978 cohort recruited in the ALSWH study in 1996, a sample of 4458 (31.3%) women were eligible for this study.
Supplemental material
Measures
Outcome measures
Outcome measures were first defined as a binary response variable of ‘yes’ if women had at least one service per calendar year (1 response) or ‘no’ if no service claim was made in the calendar year (0 response). Second, the outcome number of mental health service claims was defined as a continuous measure, and as a count measure, indicating the number of BAS services used in each calendar year which could range from 0 (no services for the year in question) to the maximum claims for the year (this varied due to government subsidy changes). Use and number of BAS services was calculated by summing the number of mental health service claims for each year. Since the Australian Medicare system provides universal coverage for all medical services to Australian citizens and permanent residents, regardless of healthcare cover it is expected that we would capture all mental health service use under the BAS. The term ‘mental health service claims’ or ‘BAS services’ used in this manuscript will refer to any of the eligible services under the BAS.
Explanatory variables
Baseline measures were obtained from survey 4 (which was surveyed in 2006 just before the introduction of the BAS initiative) which included sociodemographic and health related explanatory variables such as educational qualifications (up to year 12/posthigh school studies), area of residence (urban/non-urban living) and manage on income (not too bad, easy/impossible, difficult). Health-related factors at time of the introduction of the BAS services included self-reported comorbidities (diabetes, asthma, low iron), substance abuse in the last 12 months (yes/no), use of antidepressant medications (yes/no) and predictive factors including mental health scores from the Short Form Survey (SF-36) quality of life subscales.36 The mental health subscale (SF-36-MH) score is one of eight subscales measuring health-related quality of life. Each subscale represents a different aspect related to health status. Subscales from the SF-36 represent valid measures of physical functioning and mental health components of a patient’s health status.37 38 The eight SF-36 subscales are continuous measures that range from 0 to 100 with 0 indicating poorer health and 100 indicating better health. The SF-36-MH is created from five key questions from the Medical Outcomes Study questionnaire and can detect differences among patient groups with and without depression. It can also detect varying degrees of clinical severity. Scores of 52–60 indicated possible clinical depression and a score less than 48 correctly can classify depression.39 Silveira et al39 also argued that a score above 60 indicated an ‘unlikely clinical diagnosis’ rather than no clinical diagnosis.
MBS claims data were used to examine the number of days taken for a patient to receive their first mental health service after having a GP mental health assessment, the number of years receiving counselling treatment, the number of BAS services and types of services accessed by women.
Method of latent growth mixture model analysis
Latent class modelling has been used widely in the public health sector to model longitudinal trajectories of health behaviour patterns. Hence, latent growth mixture models (LGMM) an extension of latent class modelling, provide a powerful analytic tool to understand change over time by profiling the individual variation of service use among participants into latent classes. The LGMMs allow us to capture and quantify baseline status of the participant’s use at the start of the study and analyse the amount of change that takes place in mental health service use over time.
The fundamental latent class model represents the clustering of participants into groups determined according to the patterns of similar responses, for our study, we examine mental health service use. Latent classes describe characteristics for each class based on the participants’ class-specific response profile. The relationships between participants’ variations in observed item response patterns can be explained by the differences in latent class membership. Therefore, if participants with similar responses are grouped together to represent a specific measuring criteria, then specific strategies may be assigned to solve the outcome.40 In general, a dichotomous variable with a single item response may be explained by the following:

where p represents the unconditional probability that a participant v in the study will have a score of 1 for item i.  represents the class size parameter which indicates the unconditional probability of belonging to the latent class g. Each individual in the study may be assigned to one latent class only ensuring the sum of all class size parameters equals one. Theoretically, if a participant had a conditional probability of 1 for the item i they would be given membership into class g.
represents the class size parameter which indicates the unconditional probability of belonging to the latent class g. Each individual in the study may be assigned to one latent class only ensuring the sum of all class size parameters equals one. Theoretically, if a participant had a conditional probability of 1 for the item i they would be given membership into class g.

This simplistic formula may be extended to include continuous variables or multiple dichotomous variables to predict the latent classes. Latent class models categorise an individual into a class based on the latent class prevalence and the class-specific response probability for the items of interest. The number of classes in a model is generally determined by the fit statistics used to assess the model. The fit criteria are compared between models with different numbers of classes to select the best model to describe the data sufficiently.41
We used a variety of statistical tools to assess the best single-group model following the guidelines illustrating model acceptability. These included the goodness of fit, the model fit statistics used included the Bentler Comparative Fit Index/Tucker-Lewis Index (CFL/TLI), Bayesian Information criteria (BIC), Akaike Information Criterion (AIC) and adjusted BIC, were used to compare the relative fit for each model as the number of latent classes increased and evaluated the entropy score using the Lo-Mendell-Rubin (LMR) test (see online supplemental S2 for supporting information).
Statistical analysis strategy
The final model was selected on the basis of the fit statistics with consideration given for model convergence and ensuring that the final model did not contain correlations >1 and/or negative residual variances. In all cases multiple sets of random starting values were used to confirm that the optimal solution and estimates were reached. The number of classes was established by fitting a series of models with increasing number of latent classes and checking fit criteria. The optimal number of classes were determined by comparing the number of classes from the current model (k-classes) with the previous model (k-1 classes).
The latent variables, being the latent intercept growth factor and the latent slope growth factor, contain each participant’s propensity to use the BAS services per year. The latent outcome variable is then provided as a continuous measure having an expected value and variance. Each time a new model was executed, the latent class probabilities and the conditional probabilities were assessed for the delineation of each latent class. For this study, the entropy statistics was used to assign participants to latent classes (online supplemental S3-Latent class classification).
For each latent class descriptive statistics, the mean (SD) for continuous variables and the number and proportion for categorical variables were calculated. Lasagne plots were used to show the patterns of service use by latent classes.
Sensitivity analysis was conducted using the growth curve base model selected with baseline covariates (see online supplemental S3-Latent class growth models with covariates).
All statistical tests were performed using Mplus V.7.1 and SAS V.9.4 software.
Results
The latent growth mixture models
LGMMs were used to identify mental health service use latent classes based on the MBS claims dataset for the women (N=4458) from the 1973 to 1978 Cohort who met the inclusion criteria. Model building began with the one-class model with the greatest model improvements seen from the one-class model to the four-class model, however, continual reductions in the adjusted BIC and BIC statistics were seen for the five and six-class models. The increase in the number of latent classes resulted in an improvement in the entropy score until the four-class model, with marginal decrease in entropy score at the six-class model.
The six-class model was deemed to have better fit statistics than all other models, graphical displays of the patterns of latent class trajectories showed that timing of service use was better described by the six class model. However, this class had a marginally worst entropy than the four-class model. At each stage of analysis, the LMR test was performed to assess improved fit, with statistically significant outcomes when comparing the six-class to the five-class models (LMR: 68.77, p=0.006). The six-class model showed evidence that women’s use of the BAS services was diverse and that women had adopted and stopped the BAS services across time.
Characteristics of the women per latent class group
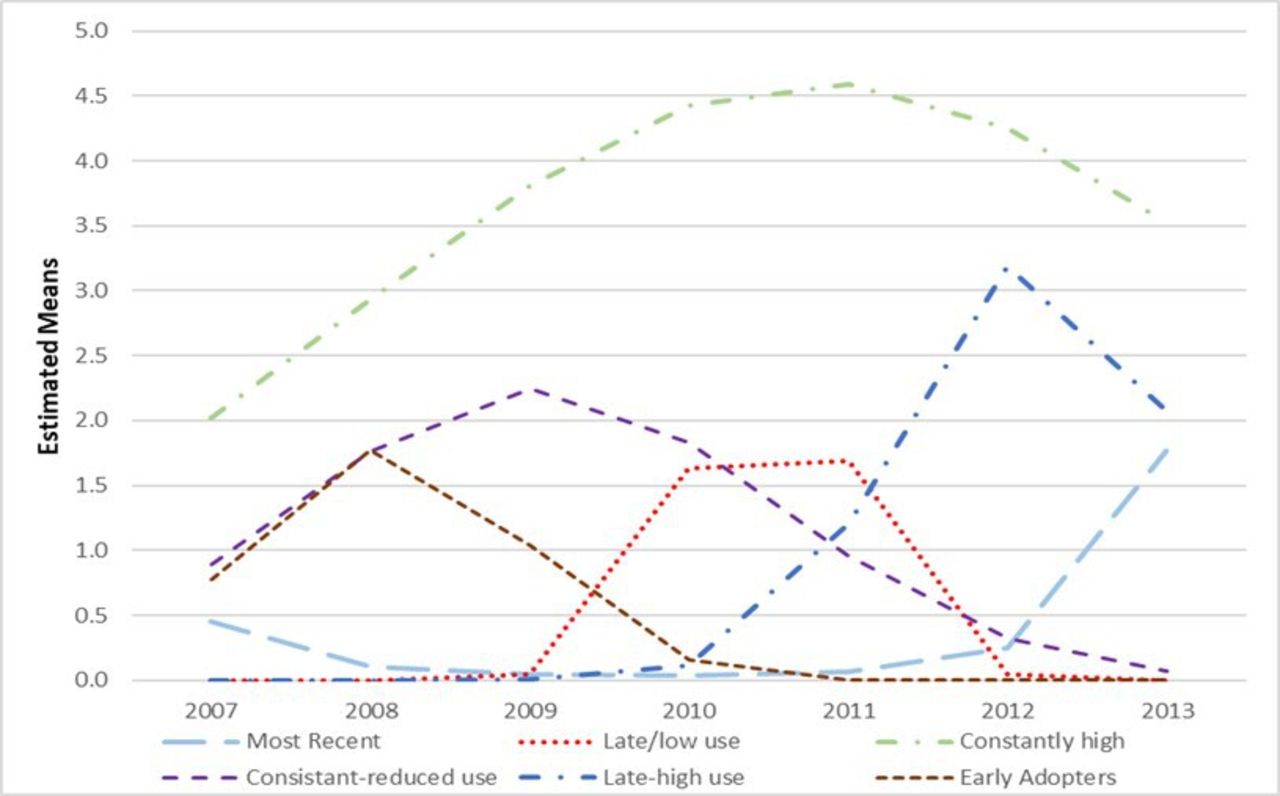
Figure 1 displays the growth component of each class and plots the estimated mean probability of use of the BAS services for each latent class by the calendar year. The ‘consistent high’ users representing women who are potentially heavy users of the mental health services each year. These 319 (7.2%) women used the BAS services consistently over 7-year period with increased use of the services during 2010–2012. Likewise, women from defined as ‘consistent-reduced’ users had consistent use of the BAS services from introduction of the BAS in 2007 to mid-way through the studies follow-up period in 2011 then reduced the use of the services in the last 2 years (N=581 (13.0%)). The trajectory of this group follows a similar pattern of consistent use of the BAS services as that of the ‘consistent high’ users but with a lower probability of use (figure 1). Women classified in ‘most recent’ users were not likely to use the services in the initial period of the study, with possible uptake of the services in 2013 (N=1179, 26.4%), showing the lowest response probability of BAS service use. Women classified in ‘early’ users, ‘late/low’ users and ‘late-high’ users show an increased use of the BAS services for a short period of time generally lasting up to 3 years (N=796, 17.9%, N=839, 18.8%, N=744, 16.7%, respectively).
Latent class membership (posterior probabilities) for the six-class model for women from the 1973 to 1978 cohort.
Table 1 shows the demographic characteristics of the groups of women who use the mental health services. Statistically significant differences exist for women of the 1973–1978 Cohort across latent classes. Women in the ‘consistent high’ users were more likely to have post-school qualifications (60% vs 54% vs 53% vs 54% vs 56% vs 52%) and live in an urban area (70% vs 60% vs 56% vs 66% vs 61% vs 55%) compared with women in the ‘most recent’, ‘late/low’, ‘consistent-reduced’, ‘late-high’ and ‘early’ classes, respectively.
Sociodemographic characteristics by latent class for women from the 1973 to 1978 cohort
In total, the ‘consistent high’ users had more GP management consultations, subsidised mental health services and used the services, on average, for more years than any other group. The ‘consistent-reduced’ and the ‘late/low’ users followed similar patterns of service use.
While mean mental health scores over time did not vary significantly across all latent profile groups, women classified ‘consistent high’ and ‘consistent-reduced’ users had lower mean mental health scores across all time points compared with all other latent classes (table 2). Mean mental health scores for women of the ‘most recent’ class had a mean decrease in mental health scores of approximately four points in 2011. This was a year before women of this profile class had their first mental health services.
Mental health service use by latent class for women from the 1973 to 1978 cohort
Figure 2 shows the patterns of service use represented by lasagne plots. At each time interval, the distribution of service use is represented by changing colours that show trajectories of participant use over time. These plots provide the patterns of mental health service use for women by latent class for each year of data collection, purple regions representing no service use and green representing service use. The graphs showing mental health service use across the six latent profile groups clearly show varied use of the BAS services by women.

{kind=link}
{kind=link}
Pattern of mental health service use by latent profile over time.
Women classified as ‘late-low’ or ‘late-high’ users of the BAS services were not likely to use the mental health services between 2007 and 2009. A greater proportion of women classified in the ‘late-low’ users were more likely to use the BAS services for approximately 1 year. Approximately 37.5% of women used the services for 2 years and a small proportion 1.9% used the services for 3 years. Women classified as ‘late-high’ users were more likely to use the mental health services in 2011–2013, with 40% of users claiming their first mental health service in 2012.
Women classified, as ‘early’ users of the BAS services were more likely to use the mental health services between the years 2007 and 2009. Only 16.3% of women used the BAS services for 2 or more years. This group of women was less likely to claim a BAS service in the later years. The ‘most recent’ users were less likely to use the BAS services in the initial years of the BAS introduction.
Discussion
The aim of this study was to examine patterns of subsidised mental health service use and subgroup women by their use. Further we aimed to examine characteristics that define women into each subgroup. It was hypothesised that over the period 2006–2012 women who used the BAS services would use them for the expected five-government allocation and that a subgroup of women would continue to use the BAS services for an additional five services. The growth mixture models profiled women’s use of the mental health services into six latent classes, which best identifies how women in the 1973–1978 cohort are using the mental health services.
Results show that the services are reaching the subpopulation of women with decreasing mental health in need of mental health services. The group of women using the services had mean mental health scores indicating possible clinical depression.39 42 Interestingly, mental health scores for these women were shown to decrease one to 4 years prior to accessing the BAS services. Treatment effects are generally noticed within 6–8 weeks after counselling services, begin,43 our study showed that for some women, mental health scores did not increase during the first year of services, rather, they continued to decline. However, improved mental health scores were noticed 1–4 years after treatment had begun. The results suggest that longer treatment periods may be essential for recovery and improved mental health varied depending on latent profile group. More importantly, long-term users showed no further decline in their mental health after commencing treatment and on average showed evidence of retaining stability in their mental health.
The integration of mental health services into primary care, was designed to allow people with mental health problems to access quality mental health services close to their homes, families and daily activities.44 Using growth mixture models our study showed that treatment use was varied and treatment patterns were diverse for the women born 1973–1978 over time. Approximately 12% of women who visited a GP about their mental health did not begin treatment offered by the BAS services. These women were profiled in the ‘early adopters’ class and may have chosen to use other counselling services not provided under the BAS or to seek no further health service support. Results of another study found that women with higher educational qualification and those living in metropolitan areas were more likely to access the mental health services offered under the BAS.4 Additionally, our study showed that by 2013, regardless of area of residence women with higher educational qualification were accessing the BAS services. Conversely, the data suggest that barriers to mental health services provided under the BAS for people living in rural areas and those with lower educational qualifications still exist, which is consistent with previous studies.4 28 35 45
People in need of mental health services are entitled to five Medicare subsidised services per year and up to 10 if required. Therefore, one of the study’s objectives was to determine the optimal number of profiles that describe women’s use of the mental health services, based on use of at least one of these services. Women were classified into six profiles based on service use over time. The latent classes identified two profiles of women with a minimum of 1-year duration of service use. In addition, three of the latent classes were accessing at least the recommended five BAS services per year, when needed. However, some women from this cohort, particularly those in the ‘consistent high’ class, have claimed more than 30 services over the 7-year period with a maximum of 201 services under the BAS. This suggests that some women are accessing more than the expected yearly government’s subsidised number of BAS services. Most women did not exceed the recommended ten BAS services which was in agreement with Pirkis et al, who found that patients were more likely to have had close to the recommended number of services.24 However, our study did add to the literature showing a small proportion of women continue to access BAS services over multiple years. Additionally, mental health service use changed for some latent groups of women corresponding to changes in the women’s mental health score overtime suggesting a continued need for BAS services, as suggested by previous other studies.29 30
The study provided evidence that women are receiving treatment based on individual needs and that different patterns of use are reflected by women’s claims for the mental health services. The data show an inequitable distribution of BAS services for women based on sociodemographic characteristics; area of residence and educational qualifications. Similar results found in another study indicated higher educational qualification and living in metropolitan areas were drivers for accessing the mental health services under the BAS.4 While there appears some inequity in the distribution of service use, they are providing integrated varied care and improved access to mental health services as intended.46 The study has captured the true number of women who accessed the BAS services, including both new and existing patients, short-term and long-term users. While it cannot specifically be inferred there is evidence that the BAS has been delivered flexibly for patients using the treatment therapies for all latent profile groups.
Treatment effects have not been assessed in this study but mean mental health scores were examined by latent class group across time. Women’s mental health showed a decline prior to use of the BAS services and improved mean mental health scores were seen across the latent profile groups after the initiation of the mental health services. Likewise, reduced use of antidepression medications was reported around the time service use declined. The analyses showed that women transitioned in and out of treatment based on their mental health needs across time and that each profile group’s patterns of use were unique to the users. This analysis supports the need to patient based treatment and tailored individual treatment.46
This study provides valuable data on the patterns of mental health service use by women from 2006 to 2013 and includes the overall proportion on types of services accessed under the BAS based on pattern of service use. Further the study highlights the need for efficient referral pathways by GPs for patients to access allied mental health treatments and ensuring the proportion of patients requiring ongoing care receive continued quality treatment.
This study is not without its limitations. First, men and women both use the mental health services, but we have only examined patterns of service use by women from the 1973 to 1978 cohort. However, another study which compared predictors to access services found that twice as many women used the BAS mental health services compared with men,28 with younger women more likely to access service compared with older women.45 Second, due to the collection periods of the ALSWH we are only able to assess change in mental health every 3 years, which may be missing significant changes in women’s mental health over that period. Additionally, the ALSWH surveys do not collect data on women’s perceived need for mental health services, and therefore, this study was not able to address gaps about lack of access. Lastly, LGMMs can be performed in a straightforward manner, a well-defined model must comply with a number of information criteria such as the AIC, BIC and entropy to ensure the overall degree of classification of stability in the model. A critical assessment of the interpretability of the selected model that classifies the latent classes is found in online supplemental S3.
Conclusion
This study has shown the importance of understanding the use of service uptake and, more importantly, provides information about this central initiative. This study examines unknown service use patterns and provides stakeholders and policymakers with a better understanding of the adequacy of the services. Further, the outcomes from the study provide evidence on the known implementation by services provided under the governance of Australia’s Medicare. We showed encouraging outcomes that service uptake had six different profiles of use. Additionally, we described characteristics of women at the time service use began for each specific profile and the flexibility that the BAS services provide for women needed to access the services. However, there still remains inequitable distribution of services for women with lower education and for those living in non-metropolitan areas.
In conclusion, we recommend to government the need to continue flexible service access when implementing new health initiatives into the community and the importance of understanding and addressing where uptake is needed.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
The ALSWH survey programme has ongoing ethical approval from the Human Research Ethics Committees (HRECs) of the Universities of Newcastle and Queensland (approval numbers H076-0795 and 2004000224, respectively, for the 1973–1978, 1946–1951 and 1921–1926 cohorts; and H-2012-0256 and 2012000950, for the 1989–1995 cohort). The ALSWH also maintains institutional HREC approvals for external record linkage (approval numbers H-2011-0371 and 2012000132, respectively). In addition, access to the MBS is approved by the Australian Institute of Health and Welfare and the Departments of Defence and Veterans' Affairs HREC.
Acknowledgments
The research on which this manuscript is based was conducted as part of the Australian Longitudinal Study on Women’s Health by the University of Queensland and the University of Newcastle. We are grateful to the Australian Government Department of Health for funding and to the women who provided the survey data. The authors acknowledge the Australian Government Department of Health for providing MBS and PBS data, and Aged Care data; and the Australian Institute of Health and Welfare (AIHW) as the integrating authority.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @XeniaDolja_Gore
Contributors Conceived and designed the study: lead author XD-G. Statistical design and input, particularly regarding methods application: XD-G and CD'E. Population health and clinical input: JEB and DL. Statistics lead, analysis and data cleaning of longitudinal linked data: XD-G. Interpretation of results and drafting the manuscript: XD-G, DL, CD'E and JEB. Responsible for the overall content as guarantor: XD-G. All authors read and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JEB and DL have received grant funding for The Australian Longitudinal Study on Women’s Health which is funded by the Australian Department of Health.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.