Article Text

Abstract
Objective To evaluate the impact of immunisation service integration to nutrition programmes and under 5-year-old paediatric outpatient departments of primary healthcare centres in Rumbek East and Rumbek Centre counties of South Sudan.
Design Retrospective intervention study.
Setting Three primary healthcare centres in Rumbek East county and three primary healthcare centres in Rumbek Centre county of Lakes state in South Sudan.
Participant We extracted the data for the uptake of pentavalent vaccine (first, second and third dose) given to children aged between 6 weeks and 23 months from immunisation records for January–June 2019 before immunisation service integration and July–December 2019 after immunisation service integration from the District Health Information System 2 website to estimate the immunisation uptake ratios and drop-out rates.
Results The uptake of the first dose of the pentavalent vaccine improved from 61% to 96% (p<0.001) after immunisation service integration into the nutrition programmes of the primary healthcare centres in Rumbek Centre county. The uptake of the second pentavalent dose improved from 37% to 69% (p<0.001) and for the third pentavalent dose from 36% to 62% (p<0.001), while the drop-out rate reduced from 57% to 40% (p<0.001). While in Rumbek East county, the uptake of the first dose of the pentavalent vaccine improved from 55% to 77% (p<0.001) after immunisation service integration into the under 5-year-old paediatric outpatient departments. The uptake of the second dose improved from 36% to 62% (p<0.001) and for the third dose from 44% to 63% (p<0.001), while the drop-out rate reduced from 40% to 28% (p<0.001). Children were 23% more likely (RR 1.23, 95% CI 1.12 to 1.36, p<0.001) to be immunised with the first dose of the pentavalent vaccine on immunisation service integration into the nutrition programmes of primary healthcare centres of Rumbek Centre county in comparison to integration into under 5-year-old outpatient departments of Rumbek East county.
Conclusion Integration of immunisation service delivery to nutrition sites and children’s outpatient departments improved the immunisation coverage and decreased drop-out rates in the Rumbek East and Rumbek Centre counties of South Sudan. This evidence of positive impact should encourage the stakeholders of the Expanded Programme on Immunisation to focus on the sustainability and scale-up of this intervention to other counties in South Sudan, as logistically as possible.
- community health services
- delivery of health care
- integrated
- health plan implementation
- child health
- communicable disease control
Data availability statement
Data are available in a public, open access repository. The immunisation coverage data used in this study is based on children eligible for pentavalent vaccination in the Rumbek East and the Rumbek Centre counties of South Sudan. Children and parents/adult carers were not involved in setting the research question or the outcome measures. These data were downloaded from the DHIS2 with approval from the ministry of health.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- community health services
- delivery of health care
- integrated
- health plan implementation
- child health
- communicable disease control
Key points
Question
This study evaluates the impact of integrating immunisation services into existing paediatric outpatient departments and nutrition programs in the primary healthcare centres of Rumbek East and Rumbek Centre counties in South Sudan.
Finding
The integration of immunisation services to nutrition programmes and paediatric outpatient departments of primary healthcare centres in Rumbek East and Rumbek Centre counties of South Sudan improved immunisation coverage and reduced drop-out rates.
Meaning
The beneficial impact of immunisation service integration to nutrition programmes and paediatric outpatient departments of primary healthcare centres in Rumbek East and Rumbek Centre counties needs to be sustained and serves as a positive example in improving immunisation coverage and reducing drop-out rates for South Sudan and beyond.
Introduction
Immunisation is the most cost-effective health intervention against deaths from vaccine preventable diseases, especially in sub-Saharan Africa.1 2 In South Sudan, vaccine preventable childhood diseases cause the largest mortality among under 5-year-old children with 251 deaths per 1000 live births, 109 deaths per 1000 live births and 99 deaths per 1000 live births in the year 1990, 2010 and 2018, respectively.3 4 While the reduction of under-5 mortality rate to 25 deaths or lower per 1000 live births by 2030 is a target of the Sustainable Development Goals as well as among the child survival targets of the government of South Sudan, current performance and trends of the health indices indicate that more time beyond 2030 will be required to achieve these targets.3 5
The health system in South Sudan has been fragile due to the cumulative years of conflict and humanitarian crises which have resulted in poor health outcomes.6–8 However, other countries with similar context including Mozambique9 10 have made significant health gains.5 11 Globally, infant mortality from vaccine preventable diseases have declined by 24% between 2010 and 2017 among under 5-year-old children, with more countries receiving polio eradication status from the World Health Organisation (WHO).12 However, the under-5 mortality rate in South Sudan has remained the same since 2010 and is significantly higher than the current under-5 mortality rate for the African continent.13 14 This is in part due to the low immunisation coverage of vaccines included in the Expanded Programme on Immunisation (EPI) in South Sudan,15 in addition to the introduction of new vaccines being limited.16 17
The official reported coverage estimates for the third dose of diphtheria, tetanus toxoids and pertussis in South Sudan from 2009 to 2019 has been around 50%.18 This is well below the coverage levels required for herd immunity19 and 74% of the country’s geopolitical counties are yet to reach 80% coverage.19 20 Addressing the poor immunisation uptake in South Sudan’s fragile environment will play a pivotal role in reversing the trend of vaccine preventable diseases and death in South Sudan. The unmet immunisation coverage is also associated with the sporadic and ongoing insecurity in some states such as the Lakes and Jonglei states.20
The joint WHO and United Nations International Children’s Emergency Fund (UNICEF) Global immunisation vision and strategy aimed at reducing mortality and morbidity from vaccine preventable diseases among under 5-year-old children. The core element of this strategy and the Immunisation Agenda 2030 involves the integration of immunisation services into other health programmes and immunising more people and social groups to improve coverage and uptake.2 21 The Immunisation Agenda 2030 provides a broad global vision and conceptual framework for vaccines and immunisation during the decade of 2021–2030, of which integration of immunisation with essential health services is one of the seven strategic priorities.21 Health service integration has proven effective in improving immunisation uptake in the outpatient department, integrated management of childhood illness, cash transfer health programmes and other integrated community case management programmes.2 22 23
In South Sudan, the current service delivery model is supported by an existing service integration policy. However, most programmes in immunisation service delivery are implemented vertically and create the integration policy-practice gap. While there are broader factors underpinning the choice of vertical or horizontal service delivery, in the context of South Sudan, horizontal (integrated) approach aligns with the South Sudan Health Pooled Fund Phase III priorities of being effective, cost-effective and equitable.24 The integrated locally owned programmes of immunisation with primary care services are effective in reducing under-5 mortality rates in South Sudan, cost-effective in being more economically and technically efficient to share resources (particularly human resources) than having them devoted to one programme disjointly, and equitable in reaching more underimmunised and zero-dose children.
In South Sudan, there is evidence of positive impact of integration on immunisation uptake in nutrition settings.25 However, evidence is lacking for under 5-year-old paediatric outpatient department settings. Our objective is to evaluate the impact of immunisation service integration to nutrition programmes and under 5-year-old paediatric outpatient departments of primary healthcare centres (PHCCs) in Rumbek East and Rumbek Centre counties of South Sudan during 2019. Specifically, we evaluated the impact for 6 months before (January–June 2019) and 6 months after (July–December 2019) immunisation service integration for the pentavalent vaccine (diphtheria, pertussis, tetanus, hepatitis B and Haemophilus influenzae type b) into the nutrition programmes of three PHCCs in Rumbek Centre county and the under 5-year-old paediatric outpatient departments of three PHCCs in Rumbek East county.
Methods
Study design and location
South Sudan consists of 10 states and 79 counties with a population of 11 062 000 people in 2019. The Lakes State includes Rumbek East and Rumbek Centre counties with a population of 153 550 and 232 752 in 2017, respectively. This was a retrospective intervention study conducted in selected PHCCs in Rumbek East county (Aduel PHCC, Pacong PHCC and Paloc PHCC) and Rumbek Centre county (Amongpiny PHCC, Malual Bab PHCC and Matangai PHCC) of South Sudan.
Immunisation service integration
Between July and December 2019, a strategy was implemented to integrate the EPI into nutrition programmes in all the PHCCs in Rumbek Centre and EPI was integrated to under 5-year-old outpatient departments in selected primary health centres in Rumbek East. The PHCCs were regularly monitored for the uptake of first, second and third dose of the pentavalent vaccine for 6 months during July–December 2019.
We refer to immunisation service integration as the adoption and assimilation of immunisation services into the nutrition service units and paediatric outpatient departments of the PHCCs wherein, the immunisation operational activities are colocated, codelivered and coreported in the nutrition service units and the paediatric outpatient departments of the PHCCs.25–27 Immunisation screening system was adopted in the nutrition service unit and the outpatient department of the PHCCs, where children between the age of 0 and 23 months were first screened for zero-dose or underimmunisation before accessing the nutrition services and the curative services. Zero-dose and underimmunised children were directed to the vaccinators for immunisation.
The intervention adopted both the functional and infrastructural service integration approaches in a synergistic relationship between the programmes’ service providers with a fully decentralised local planning context with no additional pressure from external forces.28 29 Weekly reorientation and on-job training on rapid adoption of the functional approaches and practice of service integration into their daily practice during this integration period were conducted to staff of these two programmes. As there are two implementing partners managing the nutrition service programme and the curative and preventive health services, the programme managers of these two programmes were oriented to share ownership of their programmes and ease the process of integrating immunisation services to their respective programmes. The practices adopted by these staff included staff retention practice during the period of intervention, trust between staff, staff-to-staff support, user-centred culture, shared belief and co-ownership between the two programmes’ staff, joint decision making between the two programmes’ staff and regular communication and meetings.
Vaccination schedule
The pentavalent vaccine is recommended for children at 6, 10 and 14 weeks for the first, second and third doses, respectively, as per the national immunisation schedule in South Sudan. Children who miss out on the recommended vaccination schedule are still offered the pentavalent vaccine up to the age of 2 years (less than 24 months of age).
District Health Information System
The study population includes children between 6 weeks and 23 months of age who received one, two or all three doses of the pentavalent vaccine. We extracted all of the monthly data on the pentavalent vaccine uptake from the South-Sudan’s District Health Information System 2 (DHIS2) website.30 No sampling is required since the DHIS2 dataset is representative of the general population. Also, our monitoring and supportive supervision of the vaccinators for proper recording helped in improving the data quality by ensuring completeness, accuracy and timeliness of data submission.
The records were retrieved on a monthly basis for a 12-month period in 2019 (6 months before and 6 months after intervention) across all the three monitored PHCCs in each county and was jointly checked with the county health department for data quality and validation. The data were then classified into two groups using the WHO immunisation age groups classification—infant for under 1-year-old age group (≥6 weeks and <12 months) and toddler for 1 year and above age group (≥12 months and <24 months), thereby we can compare timely coverage versus delayed coverage, respectively. Considering other confounding factors was not possible as data from the DHIS2 is restricted and limited to variables such as age, sex and geographical location of counties and communities.
Immunisation (or vaccine uptake) rate was calculated using the number of children in each targeted age group that received the last recommended pentavalent vaccine dose as the numerator, while the estimated number of target population were assumed to be the total number of surviving children in the target group for each vaccine, and was taken as denominator.31 32 Since the Southern Sudan Centre for Census, Statistics and Evaluation is yet to publish the data for the number of surviving children in the local communities of the country, we estimated the number of surviving children by subtracting estimated deaths monthly (using the country’s infant mortality rate) from the total live births per month in each county.33
Comparative effectiveness analysis
We compared the uptake for the three doses of the pentavalent vaccine before immunisation service integration intervention during January–June 2019 and after immunisation service integration into nutrition sites and children’s outpatient departments during July–December 2019, using standard normal distribution test. To address seasonally induced effectiveness bias, we also compared the intervention period (July–December) in 2019 with the same period (July–December) in 2018. Data were stratified by age and immunisation rates were obtained in each age group to adjust for the confounding effect of age. Immunisation coverage rate ratio (before and after intervention) were computed to ascertain the percentage contribution of intervention programmes in both counties. We calculated immunisation coverage rate ratio to estimate the effectiveness of the integration of the EPI in nutrition settings of Rumbek Centre county in comparison to paediatric outpatient department settings of Rumbek East county. Immunisation drop-out metric was calculated by subtracting the number of pentavalent vaccine third dose uptake from the number of the pentavalent vaccine first dose uptake in each county. The immunisation drop-out metric was divided by the uptake of the pentavalent vaccine first dose to estimate the immunisation drop-out rate.31 32 Standard normal distribution test (Z-test) was used to generate CIs (with 95% confidence level) for immunisation coverage rate ratio. Estimates with p value less than significance level (5%) were reported as strongly associated. We conducted our statistical analysis using MS Excel and SPSS V.25. The data and analysis code are publicly accessible at https://github.com/IMMUNISATION/-service-integration-immunisation-uptake to facilitate reuse of data and reproducibility of analysis.
Patient and public involvement statement
The immunisation coverage data used in this study are based on children eligible for pentavalent vaccination in the Rumbek East and the Rumbek Centre counties of South Sudan. Children and parents/adult carers were not involved in setting the research question or the outcome measures.
Results
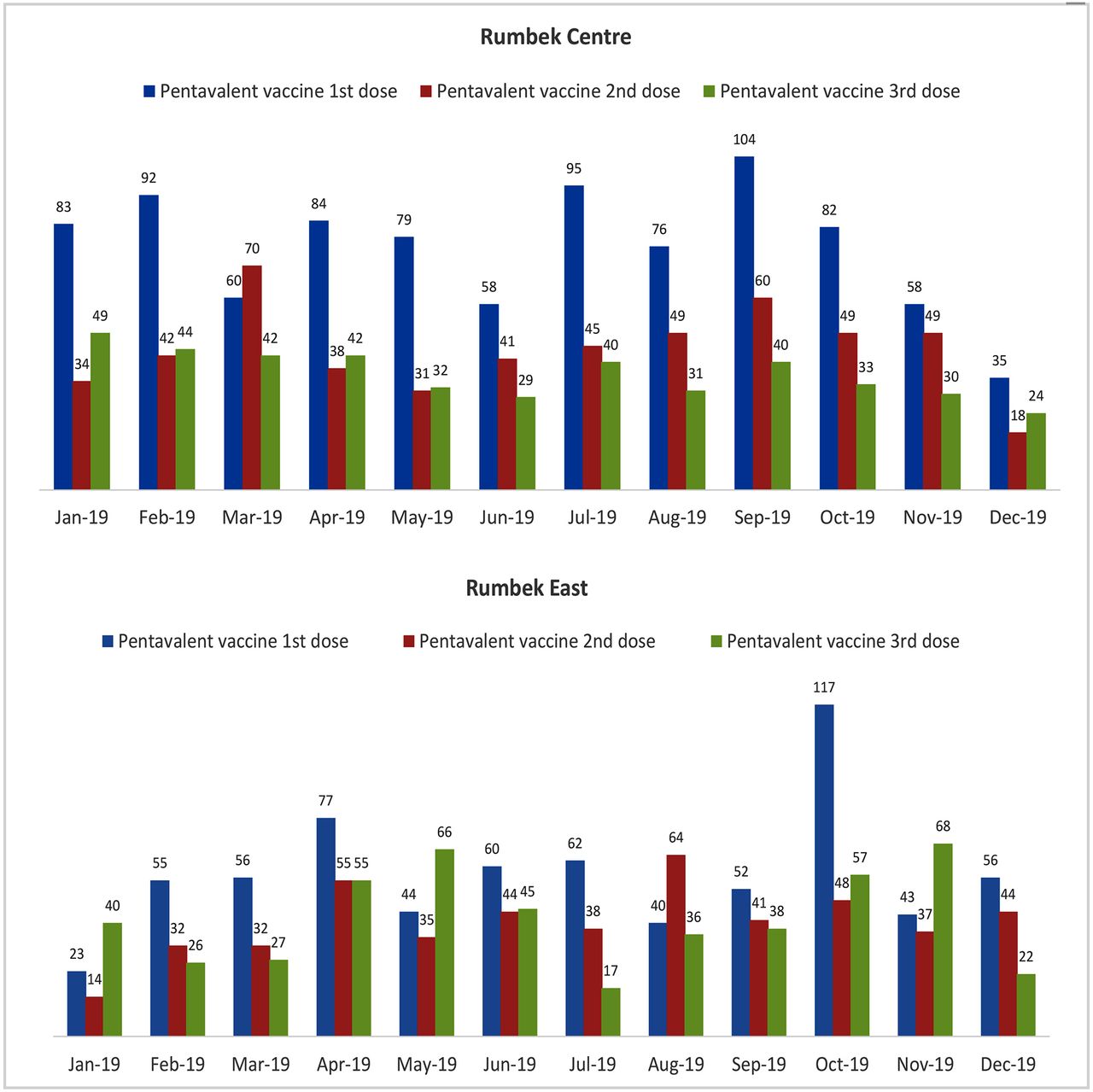
The monthly uptake of pentavalent vaccine before (January–June 2019) and after (July–December 2019) immunisation service integration into PHCCs within the nutrition programmes of Rumbek Centre county and paediatric outpatient departments of Rumbek East county are shown in figure 1.

Pentavalent vaccine uptake before and after immunisation service integration. Monthly uptake of pentavalent vaccine before (January–June 2019) and after (July–December 2019) immunisation service integration into the nutrition programmes and paediatric outpatient departments of primary healthcare centres of Rumbek Centre and Rumbek East counties, respectively. Surviving children eligible for vaccination during the preintervention and postintervention periods were 793 and 503 infants, respectively, in the Rumbek Centre county and 612 and 511 infants respectively in the Rumbek East county.
In the Rumbek Centre county, the uptake rate of the first dose of the pentavalent vaccine improved from 61% to 96% after immunisation service integration into the nutrition programmes of the PHCCs (see table 1 and figure 2). The uptake rate of the second dose improved from 37% to 69% and for the third dose from 36% to 62%, while the drop-out rate reduced from 57% to 40%. In the Rumbek East county, the uptake rate of the first dose of the pentavalent vaccine improved from 55% to 77% after immunisation service integration into the under 5-year-old paediatric outpatient departments of the PHCCs. The uptake rate of the second dose improved from 36% to 62% and for the third dose from 44% to 63%, while the drop-out rate reduced from 40% to 28%.
Pentavalent vaccine uptake rate before and after immunisation service integration

Pentavalent vaccine uptake rate before and after immunisation service integration. Pentavalent vaccine uptake rate for the three doses and drop-out rates before (January–June 2019) and after (July–December 2019) immunisation service integration into the nutrition programmes and paediatric outpatient departments of primary healthcare centres of Rumbek Centre and Rumbek East counties, respectively.
Children were 23% more likely (rate ratio of 1.23 (95% CI 1.12 to 1.36)) to have been immunised with the first dose of the pentavalent vaccine on immunisation service integration into the nutrition programmes of PHCCs of Rumbek Centre county in comparison to integration into paediatric outpatient departments of Rumbek East county (see figure 3). But there was no association of relatively higher impact of the immunisation service integration into either of these settings for the second and third doses of the pentavalent vaccine.
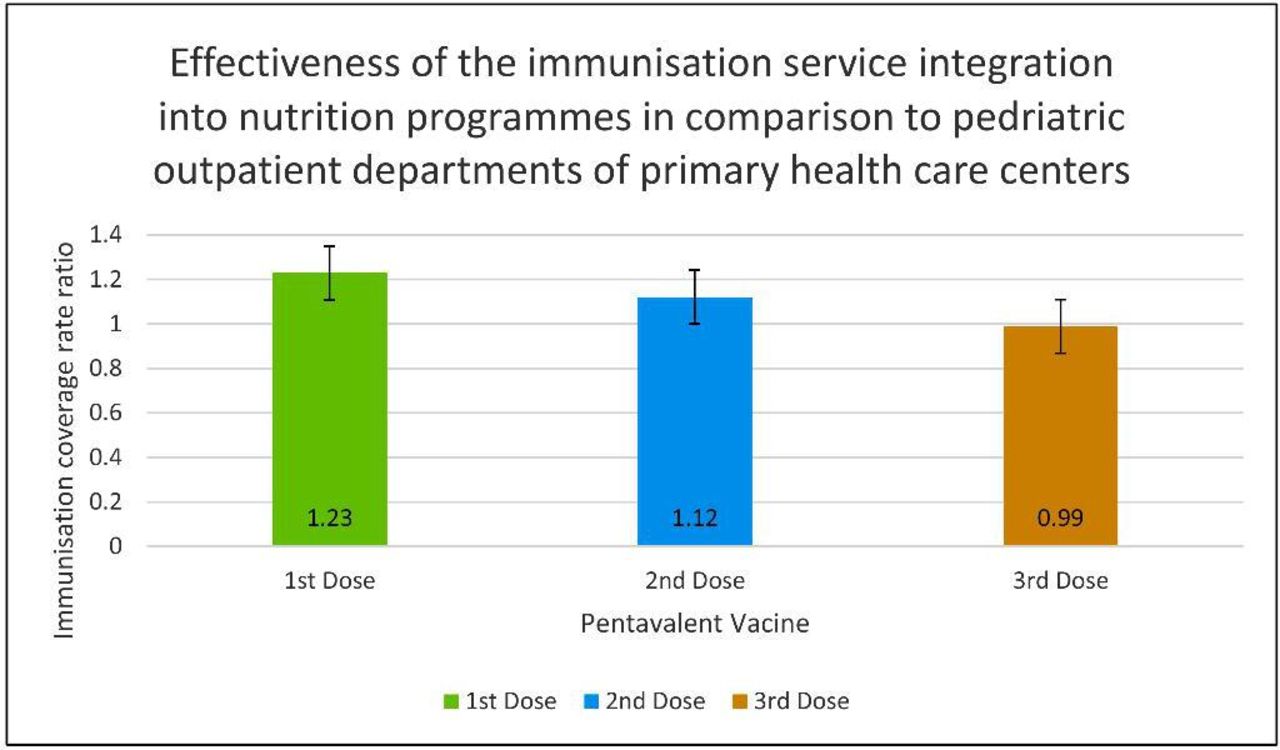
Comparative effectiveness of the immunisation service integration into nutrition programmes and paediatric outpatient departments. The effectiveness of the integration of the Expanded Programme of Immunisation into nutrition programmes of Rumbek Centre county in comparison to integration into paediatric outpatient departments of Rumbek East county (estimated through rate ratios and Z-test to generate 95% CIs) for the 1st, 2nd and 3rd doses of the pentavalent vaccine are 1.23 (1.12, 1.36; p<0.001), 1.12 (0.99, 1.26; p=0.079) and 0.99 (0.87, 1.13; p=0.394), respectively.
Generally, in the two counties, the newest birth cohort had higher vaccination coverage in comparison to previous birth cohorts (see table 2). In Rumbek Centre county, uptake rate of the first dose of pentavalent vaccine after immunisation service integration into nutrition programmes of the PHCCs, in comparison to before integration, increased from 55% to 96% (p<0.001) and decreased from 7% to 4% (p=0.369) among under 1-year-old and 1 year and above children, respectively. Similarly, the uptake rate of the second and third doses of the pentavalent vaccine among under 1-year-old children improved to 65% and 52%, respectively, postintervention in comparison to 33% and 32%, respectively, preintervention, while the uptake rate of the second and third doses of the pentavalent vaccine among 1-year-old children and above children slightly increased to 5% and 10%, respectively, postintervention in comparison to 4% and 3%, respectively, preintervention . The low coverage rate among children aged 1 year and above can also be seen in the results for Rumbek East county.
Pentavalent vaccine uptake rate before and after immunisation service integration by age
In the Rumbek East county, vaccine uptake rate of the first dose of pentavalent vaccine among under 1-year-old children improved to 75% after immunisation service integration into paediatric outpatient departments of the PHCCs in comparison to 51% before integration (see table 2). Similarly, the uptake rate of the second and third doses of the pentavalent vaccine among under 1-year-old children improved to 58% and 58%, respectively, postintervention in comparison to 34% and 40%, respectively, preintervention. The uptake rate of the pentavalent vaccine improved among children aged 1 year or above after immunisation service integration to 5% for the third dose postintervention in comparison to 4% preintervention. The drop-out rates are significantly lower among the above 1-year-old children postintervention in comparison to preintervention in Rumbek East county.
To address seasonally induced effectiveness bias, we also compared the impact during the postintervention period of July–December 2019 with the preintervention period of July–December 2018. We observed improvements in pentavalent vaccine coverage similar to the comparative analysis for the period before (January–June 2019) immunisation service integration and after (July–December 2019) immunisation service integration (see tables 3–4 and figure 4), except that the improvement in the second dose coverage was not significant in both Rumbek Centre and Rumbek East counties.
Pentavalent vaccine uptake rate before and after immunisation service integration (accounting for seasonality bias)
Pentavalent vaccine uptake before and after immunisation service integration by age (accounting for seasonality bias)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pentavalent vaccine uptake rate before and after immunisation service integration (accounting for seasonality bias). To address seasonally induced effectiveness bias, pentavalent vaccine uptake rate for the three doses and drop-out rates before (July–December 2018) and after (July–December 2019) immunisation service integration into the nutrition programmes and paediatric outpatient departments of primary healthcare centres of Rumbek Centre and Rumbek East counties, respectively.
Discussion
Our study findings show that integration of immunisation into outpatient therapeutic programme centres and nutrition programmes improved immunisation coverage and reduced drop out rates. Children were more likely to be immunised with the first dose of pentavalent vaccine after immunisation service integration into the nutrition programmes of the PHCCs compared with integration into paediatric outpatient departments. However, no association was observed for the second and third doses of the pentavalent vaccine. Additionally, this study observed low immunisation coverage among children above 1 year compared with children below 1 year.
Similar inferences have been highlighted in prior studies on the benefits of integrating the EPI with comprehensive health service delivery and recommending broader adoption in South Sudan.25 26 34 35 In the Rumbek Centre county, our inferences on improved immunisation coverage through integration into nutrition programmes are supported by findings by Oladeji et al in a similar study25 conducted in the Liech state of South Sudan which also found increased childhood immunisation coverage and reduced drop-out rates. The study also highlighted a higher adherence to vaccination among children vaccinated at outpatient therapeutic programme centres in comparison to PHCCs. Similar supportive evidence has been generated by related studies with a positive impact on nutrition outcomes36 and that nutrition counselling and education improved coverage of the third dose of the diphtheria, pertussis and tetanus (DPT3) vaccination by 68%.37 Since nutritionists assessed the immunisation status of the children before enrolling them in the nutrition programme, this ensured that missed opportunities for immunisation were assessed and counselled. Also, integration has been successful the other way around as well when other interventions such as vitamin A supplementation to immunisation campaigns have improved immunisation coverage.38
In the Rumbek East county, the improvement in immunisation uptake can be attributed to regular monitoring, motivation and health education in the paediatric outpatient departments of PHCCs. Also, mothers/caregivers would like to vaccinate their children in an outpatient clinic where they can access free treatment, and most mothers who deliver in the clinic receive adequate antenatal care which could increase immunisation uptake as well. These findings are corroborated by a systematic review on childhood immunisation interventions in low-income and middle-income countries, which found that facility-based health education plus redesigned vaccination reminder cards in outpatient departments improved coverage of DTP3 vaccination by 50%.37 On the other hand, we believe that the impact of the intervention in Rumbek East county was thwarted by a communal conflict between the two major communities—Pacong and Aduel communities from August to September 2019. However, some of the children who missed their immunisation schedule as a result of reduced access and uptake of immunisation and nutrition services due to displacement or fear of mobility were traced and vaccinated using a supplementary immunisation strategy in the month that followed the crisis. This can be seen in the spike of pentavalent first dose uptake of Rumbek East county in October 2019 (see figure 1).
We observed reduction in immunisation drop-out rates after integration in both nutritional programmes and paediatric outpatient departments of PHCCs. Similar reductions in drop-out rates have been recorded among children attending a paediatric outpatient clinic at Juba Teaching Hospital in 201739 and in a health facility-based study conducted in South Sudan.40 The missed opportunities for immunisation were relatively similar in both Rumbek Centre and Rumbek East counties after immunisation service integration.
The distance to access immunisation services is a good predictor of vaccination coverage in low-income and middle-income countries. Low vaccination coverage has been reported among caregivers living farther away from the health facilities if no growth monitoring programmes and incentives were provided. This finding is consistent with a study in Zambia which showed that immunisation uptake was lower among caregivers living further away from the health facility before a growth monitoring programme was introduced into the immunisation services.41 The barrier posed by longer travel distances to access immunisation especially for the second and third doses of the pentavalent vaccine could be partially addressed through incentives to attend the PHCCs in both Rumbek East and Rumbek Centre counties.
Immunisation uptake of the first, second and third doses of the pentavalent vaccine was higher among under 1-year-old children in comparison to children aged above year in both the Rumbek East and Rumbek Centre counties. In West Cameroon, a study showed similar findings where immunisation coverage of the pentavalent vaccine decreased as the children’s ages increased.42 Although we did not assess the factors associated with low coverage among children aged above 1 year, other studies have reported limited parental knowledge on child health management, fragile vaccination health services, geographical limitations, economic struggle, mother’s level of education and cultural accessibility as the major reasons for the low uptake.42 43 We hypothesise that the high child care burden of the mothers due to high fertility rates coupled with other household chores, poor community sensitisation and internal displacement contributed in part to the low immunisation rates among older children.
While childhood immunisation coverage among under 5-year-old children in low-income and middle-income countries is below the global average, the coverage is relatively even lower in South Sudan especially in the conflict affected areas.25 The EPI was initiated in 1974 by the WHO and United Nations International Children’s Emergency Fund44 through a vertical approach which later shifted to an integration approach by integrating immunisation services with other health services within the Integrated Management of Childhood Illness context.45 The reasons for WHO’s recommendation for horizontal integration of childhood immunisation with other health programmes are improved efficiency and cost savings.46 This stems from a decrease in competition for resources and duplication of the health systems in comparison to vertical programmes. Immunisation service integration also has challenges, such as overburdened healthcare staff, unequal resource allocation, difficult funding mechanism, donor policies and logistical difficulties.23 Therefore, the benefits inferred in this study for immunisation service integration with nutrition programmes and paediatric outpatient departments in PHCCs will need to be assessed against the risks imposed by operational logistics and compatibility differences between health programmes for successful integration.27
The nutrition services in our study were planned to facilitate codelivery and a shared-information approach was used to ensure that all the services were provided at the nutrition centre. Children’s nutrition status and growth monitoring are important to mothers and caregivers and hence the drive to attend nutrition services delivery programmes.47 Consequently, nutrition services such as growth monitoring, nutrition counselling and education were placed as core services while immunisation services were also conducted. This highlights the benefits of integrating immunisation services into nutrition programmes to improve the childhood immunisation coverage, as inferred by our study through increased uptake of the pentavalent vaccine. Sustaining community-based activities is a major challenge in low-income and middle-income countries.41 47 In our study, the nutrition programmes at the PHCCs of Rumbek Centre county provided nutritional incentives for the community. Provision of incentives especially in community programmes has been shown to be effective in motivating communities, improving effectiveness and impact of the programmes.48
In the paediatric outpatient departments, recipient-oriented interventions such as recalls and reminders, health education, teaching recipients’ skills and provider-oriented interventions such as health services audits and feedback mechanism, chart based or calendar reminders were also provided. While we infer in our study the increased uptake of the pentavalent vaccine, this also highlights the benefits of integrating immunisation services into paediatric outpatient departments to improve childhood immunisation coverage. Immunisation service integration into both nutrition programmes and paediatric outpatient departments of PHCCs have effectively reduced missed opportunities for vaccination.
Under normal operations of the vertical immunisation programme in South Sudan, after visiting the nutrition or outpatient departments in the PHCCs, mothers were asked to visit the immunisation unit which is located 30 m or longer from their current service delivery point. However, most mothers who were referred to the immunisation unit refrain from immunising their children during the same visit to the PHCCs due to the following barriers. Mothers report (1) being tired after waiting for long hours in the nutrition or outpatient departments, (2) vaccinators not being present at the time they go for vaccinations, (3) being asked to queue again after spending long hours in other nutrition or outpatient departments, (4) urgent need to return home to their domestic activities and (5) getting late to go home. As highlighted in this study, by integrating the immunisation services to the nutrition and paediatric outpatient departments of the PHCCs in Rumbek East and Rumbek Centre counties of South Sudan, mothers did not have to queue again since vaccinators were also present at the point of service delivery in the nutrition and paediatric outpatient departments.
As future directions, cost-effectiveness studies are needed to facilitate decision making and prioritisation of immunisation service integration into nutrition programmes and paediatric outpatient departments while considering the contextual characteristics of workers' training, stakeholders support, vaccine supply chain constraints and community demand for vaccination. With South Sudan emerging from protracted civil wars, we infer a favourable impact of immunisation service integration into nutrition programmes and paediatric outpatient departments in this study. This highlights a positive way forward to optimise and scale-up the integration of the EPI with other health services in the PHCCs to improve childhood immunisation coverage in South Sudan.
Our study has limitations, including the study duration being relatively short in comparison to other studies done on immunisation service integration.25 We acknowledge that a time lagged study could have improved the robustness of the study results. We also acknowledge that considering other predisposing factors such as age and sex of the child, mothers’ sociodemographics, lifestyle and knowledge about immunisation41 would be informative and could influence immunisation uptake. Further, the impact of immunisation service integration could have been influenced by the close monitoring of the immunisation service delivery by both the immunisation managers and nutrition workers.
Conclusion
In summary, immunisation service integration to nutrition programmes and paediatric outpatient departments of PHCCs in Rumbek East and Rumbek Centre counties of South Sudan during 2019 has improved the uptake of the pentavalent vaccine and reduced the drop-out rates. This positive impact favours policy and practice changes to optimise and scale-up the integration of the EPI with other health services in the PHCCs to improve childhood immunisation coverage and equity while reducing morbidity and mortality from vaccine preventable infectious diseases among under 5-year-old children in South Sudan.
Data availability statement
Data are available in a public, open access repository. The immunisation coverage data used in this study is based on children eligible for pentavalent vaccination in the Rumbek East and the Rumbek Centre counties of South Sudan. Children and parents/adult carers were not involved in setting the research question or the outcome measures. These data were downloaded from the DHIS2 with approval from the ministry of health.
Ethics statements
Ethics approval
Ethics approval for this study was granted by the Health Research Ethics Committee of the State Ministry of Health (SMoH) of Lakes State (formerly Western Lakes State), South Sudan (Reference number: MOH/WLS/14/09/2019).
Acknowledgments
We thank the Expanded Programme for Immunisation Operation team of the State Ministry of Health, Western Lakes State of South Sudan for their involvement and support of the immunisation service integration into the existing nutrition and under 5-year-old paediatric outpatient department programmes. We thank the clinical officers, vaccinators and nutrition workers who participated in the study. We also acknowledge Olusola Oladeji and his team for also providing evidence in support of immunisation service integration in South Sudan. KA is supported by the Vaccine Impact Modelling Consortium (OPP1157270).
References
Footnotes
Contributors IOI conceptualised this study, supervised the implementation of the intervention, organised data management, planned the methodology, analysed the data and led the report writing. SAL planned the methodology, participated in data management, analysed the data and participated in report writing. JT participated in data analysis and report writing. KA was involved in study conceptualisation, participated in data analysis and report writing. VAO was involved in the study conceptualisation and report writing. JGO was involved in the study conceptualisation, supervised the implementation of the intervention and report writing.
Funding KA is supported by the Vaccine Impact Modelling Consortium (OPP1157270).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.