Article Text

Abstract
Objectives To examine the factors associated with COVID-19 vaccine receipt among healthcare workers and the role of vaccine confidence in decisions to vaccinate, and to better understand concerns related to COVID-19 vaccination.
Design Cross-sectional anonymous survey among front-line, support service and administrative healthcare workers.
Setting Two large integrated healthcare systems (one private and one public) in New York City during the initial roll-out of the COVID-19 vaccine.
Participants 1933 healthcare workers, including nurses, physicians, allied health professionals, environmental services staff, researchers and administrative staff.
Primary outcome measures The primary outcome was COVID-19 vaccine receipt during the initial roll-out of the vaccine among healthcare workers.
Results Among 1933 healthcare workers who had been offered the vaccine, 81% had received the vaccine at the time of the survey. Receipt was lower among black (58%; OR: 0.14, 95% CI 0.1 to 0.2) compared with white (91%) healthcare workers, and higher among non-Hispanic (84%) compared with Hispanic (69%; OR: 2.37, 95% CI 1.8 to 3.1) healthcare workers. Among healthcare workers with concerns about COVID-19 vaccine safety, 65% received the vaccine. Among healthcare workers who agreed with the statement that the vaccine is important to protect family members, 86% were vaccinated. Of those who disagreed, 25% received the vaccine (p<0.001). In a multivariable analysis, concern about being experimented on (OR: 0.44, 95% CI 0.31 to 0.6), concern about COVID-19 vaccine safety (OR: 0.39, 95% CI 0.28 to 0.55), lack of influenza vaccine receipt (OR: 0.28, 95% CI 0.18 to 0.44), disagreeing that COVID-19 vaccination is important to protect others (OR: 0.37, 95% CI 0.27 to 0.52) and black race (OR: 0.38, 95% CI 0.24 to 0.59) were independently associated with COVID-19 vaccine non-receipt. Over 70% of all healthcare workers responded that they had been approached for vaccine advice multiple times by family, community members and patients.
Conclusions Our data demonstrated high overall receipt among healthcare workers. Even among healthcare workers with concerns about COVID-19 vaccine safety, side effects or being experimented on, over 50% received the vaccine. Attitudes around the importance of COVID-19 vaccination to protect others played a large role in healthcare workers’ decisions to vaccinate. We observed striking inequities in COVID-19 vaccine receipt, particularly affecting black and Hispanic workers. Further research is urgently needed to address issues related to vaccine equity and uptake in the context of systemic racism and barriers to care. This is particularly important given the influence healthcare workers have in vaccine decision-making conversations in their communities.
- preventive medicine
- public health
- COVID-19
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Anonymous data are publicly available on Open Science Framework (OSF) data repository with the persistent URL: https://osf.io/mhnrp/.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The primary outcome is COVID-19 vaccine receipt rather than intention of receipt.
The large sample size permitted analysis by diverse demographic and occupational subgroups.
The study has some limits in generalisability given the setting is in New York City and a representation from an academic health system.
The high rate of COVID-19 vaccine receipt may be the result of response bias.
Introduction
The equitable uptake of effective vaccines against SARS-CoV-2 will be critical to control the COVID-19 pandemic. Approval of the first COVID-19 vaccines in the USA was preceded by months of intense public and political discourse on potential vaccine efficacy and safety. Throughout 2020, estimates of COVID-19 vaccination intent in the general adult population ranged from less than half to approximately three-quarters, and pointed to an urgent need to address vaccine confidence.1 Members of groups affected by systemic racism suffered disproportionate morbidity and mortality during the COVID-19 pandemic.2–7 These groups, in particular black individuals, have long suffered gross abuses and injustices in healthcare. Partly as a result, members of marginalised groups have expressed lower intent to receive COVID-19 vaccines.2 8 9
In December 2020, the first COVID-19 vaccines were authorised for emergency use in the USA and healthcare workers were among the first groups to be offered the vaccines.10 Recent working papers have highlighted the need to effectively engage local communities in COVID-19 vaccination11 and to equitably distribute the vaccines.12
Globally, local healthcare workers are some of the most trusted and influential professionals in individual and family decisions around vaccination.13 14 Beyond their work roles, healthcare workers are also influential members of the communities in which they live. Vaccine hesitancy is prevalent among healthcare workers globally.15 The WHO emphasises that targeted discussions and engagement with healthcare providers will be essential to obtaining widespread vaccination confidence, as they will be the first ones expected to get the vaccine and they will be on the front lines facing questions from the public.16 Here, we examine the demographic, work role and vaccine-related belief factors associated with COVID-19 vaccine receipt among healthcare workers during the initial roll-out of the COVID-19 vaccine in a diverse region of New York City heavily impacted by the pandemic.
Methods
Setting
We conducted an online cross-sectional survey (see online supplemental file 1) of healthcare workers at two large integrated healthcare systems (one public and one private) in New York City. COVID-19 vaccines were available in New York City beginning 14 December 2020. Based on New York State guidelines, healthcare workers at high risk of exposure were in the first COVID-19 vaccine eligibility category. Vaccine eligibility expanded throughout our data collection time period.
Supplemental material
Supplemental material
For participant eligibility, we defined healthcare worker broadly to include physicians, nurses, allied health professionals, advanced practice providers, environmental services workers, community-based providers and researchers/educators. We recruited participants through use of hospital listservs, newsletters and emails, and through distributing posters and flyers on-site at locations across the health systems. The survey was distributed only within the health systems’ networks and visible only to employees. The survey was available in English, Spanish, Bangla, Mandarin, Nepali and Haitian Creole. We offered an incentive for a chance to win one of ten $50 cash prizes. The survey was available electronically via REDCap and by paper on request.
The online form included exclusively forced choice questions, except for two open-ended questions with free-text answers included at the end of the survey. As such there were no missing data. We also offered paper surveys, which were completed by nine participants. We did not include them in the primary analysis as the data were incomplete or clearly inaccurate. We removed duplicate surveys from the analysis.
Data collection ran from 23 December 2020 to 16 February 2021, corresponding to the first 2 months of the COVID-19 vaccine roll-out.
Main measures
We asked respondents if they had been offered a COVID-19 vaccine by the time of the survey, and if offered whether they received one, along with other questions pertaining to influences of vaccine beliefs and behaviours (see online supplemental file 1). We did not ask respondents if they received more than one dose. To measure general vaccine confidence, we used the Vaccine Confidence Index (VCI), which was developed and validated by The Vaccine Confidence Project to measure ‘individual perceptions on the safety, importance, effectiveness, and religious compatibility of vaccines’.17–19 The following are the three statements: ‘Overall, I think vaccines are safe’, ‘I think vaccines are important for children to have’ and ‘Overall, I think vaccines are effective’. For computing the VCI as a numerical score, we assigned numerical values to responses to each of the three questions (strongly agree=5, somewhat agree=4, neither agree nor disagree=3, somewhat disagree=2, strongly disagree=1). While there is, as yet, no standardised way of categorising responses, we used existing literature20 and visual inspection of the data to assign VCI scores less than 9 as low vaccine confidence. We used Brewer et al’s21 model of vaccination behaviour to develop questions that measured perceived COVID-19 disease risk, COVID-19 vaccine benefits and COVID-19 vaccine harms. We included two optional open-ended questions at the end of the survey inviting participants to share their thoughts and suggestions and what resources would help them provide information about COVID-19 with more confidence.
Quantitative analytical methods
We report COVID-19 vaccine receipt by demographic and occupational factors, general vaccine confidence, influenza vaccine receipt and COVID-19 vaccine attitudes. We expressed results in the form of means, proportions and 95% CIs. We conducted bivariate analyses using Χ2 tests for categorical variables and Wilcoxon rank-sum tests for the continuous variable VCI, with significance set at α=0.05. For this analysis focused specifically on vaccine receipt (rather than intent) as the primary outcome, respondents who had not yet received the vaccine but planned to get it were included in the ‘no’ category.
We developed a multivariable logistic regression model to assess the adjusted and relative contributions of demographic variables and vaccine confidence on COVID-19 vaccine receipt when offered. For the logistic regression model, we used the Lasso procedure22 in R Studio V.1.4.1103, which uses regularisation, cross-validation and penalisation to identify important predictor variables and improve the interpretability and predictive accuracy of the final statistical model. We used 50% of the data set23 for training and 50% for testing. Independent variables inputted into the model included demographic variables, occupational variables and workers’ perceptions of COVID-19 vaccine benefits, harms and disease risk (see online supplemental file 2). For generating ORs and CIs in the final model, we used the glm procedure in R.
Supplemental material
Qualitative analytical methods
We analysed the free-text survey response data through summary descriptive statistics. Review of survey response transcripts allowed for preliminary thematic analysis to formulate detailed narratives. Open coding of survey transcripts was completed by two team members (AC, LS), which led to an initial set of codes, which were refined by a third member (RM). These were organised according to themes that emerged from the data. We generated a codebook of code definitions and examples. We completed coding of all transcripts completed by two team members using Dedoose software (SocioCultural Research Consultants, Manhattan Beach, California, USA). We formulated the final set of overarching themes in discussion with the full study team. An additional reviewer (AH) assessed each statement for theme content and established frequency tables of theme content by demographic variables. Illustrative quotes pertaining to commonly reported themes were extracted from the data and documented.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our research. We plan to disseminate the results of our study to healthcare workers and stakeholders at participating institutions using infographics, summary reports and presentations.
Results
Study population
Between 23 December 2020 and 16 February 2021, 2191 healthcare workers attempted and 2109 (96%) completed the survey. Among participants who completed the survey, 1933 (92%) had been offered the COVID-19 vaccine at the time of survey completion. We restricted our analysis to this group (see demographics in table 1).
Participant characteristics by receipt of COVID-19 vaccine when offered
Vaccination receipt rate
Of the respondents who were offered the vaccine, 81% reported they had received a COVID-19 vaccine, 11% reported they plan to get it but had not scheduled or gone for the vaccine yet, and 8% had not received the vaccine (table 1). COVID-19 vaccine receipt was highest among men, respondents aged less than 40 years and 60 years or older, and white respondents. By role, physicians (95%), researchers/educators (92%) and advanced practice providers (92%) were the most likely to be vaccinated, while community-based health workers were the least likely to have received the vaccine (29%). Among healthcare workers who reported receiving an influenza vaccine, 84% also received the COVID-19 vaccine compared with 44% of healthcare workers who did not receive a seasonal influenza vaccine (p<0.001).
Perception of COVID-19 vaccine benefits
Healthcare workers who agreed with statements about the COVID-19 vaccine’s importance in protecting family members were more likely to receive the vaccine compared with those who did not agree with this statement (86% compared with 25%, p<0.001). This relationship was consistent across workers with different beliefs in the vaccine’s importance in protecting community members, coworkers and patients. Table 2 presents the bivariable analysis of vaccine receipt by vaccine beliefs and risk appraisal.
Risk appraisal, beliefs and media behaviours by receipt of COVID-19 vaccine
Perception of COVID-19 vaccine risks
Regarding potential COVID-19 vaccine risks, 27% of the respondents expressed concern about being experimented on, 40% expressed concern about vaccine safety and 48% expressed concern about side effects (see online supplemental file 3 for beliefs by race or ethnicity). Among respondents who expressed concern about safety, 64% received the vaccine, as did 70% with concerns about side effects, compared with 92% of respondents who did not express those concerns (p<0.001). Respondents who expressed concern about being experimented on were less likely to have received the vaccine compared with those who did not (57% compared with 90%, p<0.001). Black respondents in a non-physician or academic role were more likely to be concerned about being experimented on than their white colleagues (over 60% compared with less than 25%; see figure 1). Among all participants, 94% of the respondents agreed that ‘overall, vaccines are safe’ and 93% received the influenza vaccine during the most recent influenza season (2020–2021).
Supplemental material

Per cent of respondents strongly or somewhat agreeing with the statement ‘I am worried about being experimented on’, by race and ethnicity.
COVID-19 disease risk appraisal
Across participants, 80% believed they were at high risk of getting COVID-19 due to their job. Healthcare workers who felt they were at high risk due to their job were more likely to have received the vaccine (83% compared with 75%, p<0.001). Among those who disagreed that their job put them at high risk, 69% still reported vaccine receipt. Being at high risk for COVID-19 complications due to underlying health conditions did not affect vaccine uptake (79% compared with 82%, p=0.07). Healthcare workers who responded that they did not need the vaccine because they had a history of COVID-19 or had positive antibodies represented 6% of the total participants but made up 21% of participants who did not receive the vaccine.
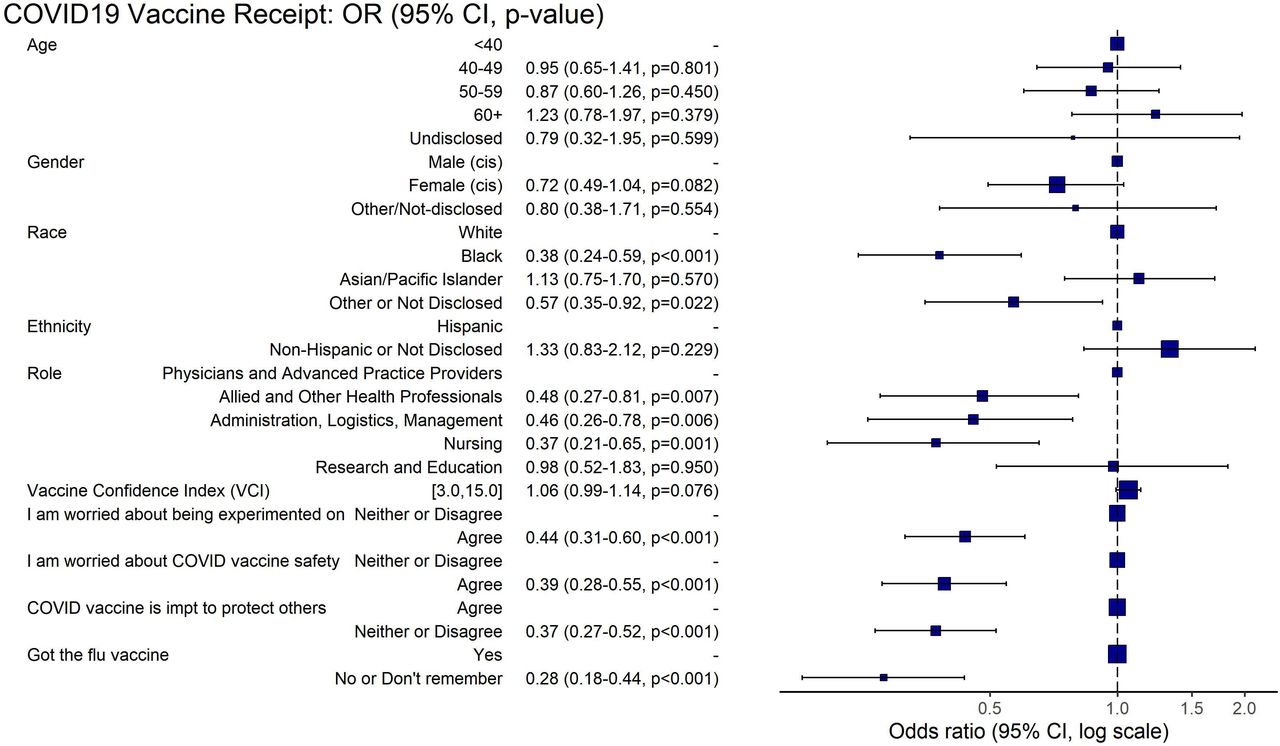
Multivariable analysis
The final multivariable model is shown in figure 2 (see online supplemental file 2 for coefficients). Identifying as black was associated with a decreased vaccine receipt (OR 0.38, 95% CI 0.24 to 0.59). Concerns about vaccine safety and being experimented on continued to predict lower vaccine receipt (OR 0.39, 95% CI 0.28 to 0.55 and OR 0.44, 95% CI 0.31 to 0.60). Beliefs in the importance of the vaccine protecting others remained associated with higher vaccine receipt (OR 2.69, 95% CI 1.93 to 3.74). By occupational category, a role in nursing (OR 0.37, 95% CI 0.21 to 0.65), administration (OR 0.46, 95% CI 0.26 to 0.78), or allied and other health professionals (OR 0.48, 95% CI 0.27 to 0.81) remained significant for decreased odds of vaccine receipt compared with physicians and advanced practice providers. Influenza vaccine receipt (OR 3.57, 95% CI 2.30 to 5.56) was also associated with higher odds of COVID-19 vaccine uptake. Higher general vaccine confidence measured by the VCI (OR 1.06, 95% CI 0.99 to 1.14, p=0.076) was not significant in the final multivariable model (see online supplemental file 4 for VCI by role and race/ethnicity).
Supplemental material

{kind=link}
{kind=link}
Multivariable logistic regression model on the predictors of COVID-19 vaccine receipt.
Trusted sources of COVID-19 vaccine information and social media patterns
When asked ‘who do you trust MOST to give you advice on COVID-19 vaccines?’, 39% of healthcare workers chose ‘my primary care doctor’, followed by ‘federal government agencies’ (28%) and ‘other healthcare professionals’ (12%). Physicians and advanced practice providers were more likely to report ‘federal government agencies’ (36%), followed by their primary care doctor (23%). Among healthcare workers who did not get the COVID-19 vaccine by the time of survey completion, the most trusted source was also their primary care doctor (49%), followed by federal government agencies (16%) (see online supplemental file 5). When asked ‘how much do you trust advice on COVID-19 vaccines’ from different sources, unvaccinated healthcare workers were less likely to choose ‘a lot’ for any of the sources. Across all sources for advice, black healthcare workers were more likely to choose ‘not much’ or ‘not at all’ (see online supplemental file 6).
Supplemental material
Supplemental material
Healthcare workers reported they were asked their opinion about COVID-19 vaccination multiple times in the past month by coworkers (73%), family members (86%) and community members or friends (73%) (see online supplemental file 7).
Supplemental material
Qualitative results
Overall, 641 respondents provided free-text answers to the open-ended questions at the end of the structured survey. Of these respondents, 459 (72%) were female, 142 (22%) were male and 40 (6%) were queer/non-binary, transgender female-to-male (FTM), other gender, or preferred not to identify their gender. We summarise the qualitative results of the free-text responses in table 3. Statements aligning with the theme of mistrust in the vaccine were more frequently cited among healthcare workers who identified as black, and black healthcare workers provided reasons for hesitancy more frequently than other racial/ethnic groups (see online supplemental file 8). Participants’ ‘suggestions for mass vaccination and distribution’ included logistical improvements for vaccine sites, transparency in distribution, providing incentives for vaccination and ideas regarding the order of eligibility. In response to the prompt for suggested tools and resources, participants had a variety of suggestions for what is needed regarding vaccine education and confidence promotion. The identification of educational needs was the most frequently endorsed theme.
Supplemental material
Qualitative analysis summary table of free-text survey responses
Discussion
We found that while COVID-19 vaccine uptake among healthcare workers in our study is the norm—81% of respondents received the vaccine—there were important inequities in vaccine receipt by race, gender, age and healthcare worker role. Our study, occurring in the immediate 2-month period following vaccine roll-out among healthcare workers, is among the first to report COVID-19 vaccine receipt rather than intent, and to investigate the association of COVID-19 vaccine receipt with vaccine confidence and perceptions of vaccine risks and benefits among healthcare workers. Our rate of COVID-19 vaccine uptake is similar to other studies, which ranged from 80% to 96%.24–28
Our results on race support findings from earlier research that examined COVID-19 vaccine intent prior to vaccine availability, including among healthcare workers.29–36 Consistent with early reports of COVID-19 vaccination rates in the USA, we found black and Hispanic participants were less likely to receive the COVID-19 vaccine at the time of our survey. The Centers for Disease Control and Prevention reported that among persons who received the vaccine, the proportion who identified as black was lower than would be expected based on eligibility.37 Similarly, in New York City at the time of our study, black New Yorkers made up 12% of vaccine recipients, but 24% of the population.38 Both reports were limited by incomplete data collection for race and ethnicity, but in our sample 94% of the respondents reported race/ethnicity data.
We found higher perceived benefits of COVID-19 vaccination for protecting others had the largest effect size in predicting vaccine receipt. Lower perceived vaccine harms including safety and being experimented on also predicted vaccine receipt. Higher perceived benefits of COVID-19 vaccination, higher perceived risk of COVID-19 disease and more positive attitudes towards vaccination have been associated with greater intent to vaccinate in the general US population and among healthcare workers worldwide.1 31 33 39 A similar study among emergency department and emergency medical services (EMS) staff in the USA found higher perceived COVID-19 vulnerability was associated with early vaccine uptake.26
A prior study investigating COVID-19 beliefs, vaccine intent and race found that beliefs mediate the association of race and vaccine intent.40 Here, black healthcare workers had lower COVID-19 vaccination rates even after accounting for safety concerns and provaccine beliefs in the multivariable model. Vaccine intent does not always translate to vaccine receipt21 and this effect may be greater among black healthcare workers. While all healthcare workers in this study had been offered the vaccine in their workplaces, there may have been racial differences in actual access (eg, ability to take time off duty to wait for the vaccine) which our study was not designed to detect. The effects of systemic racism, the history of research abuses among people of colour in the USA and the lived experience of mistreatment in healthcare systems likely all contribute to lower trust and vaccination rates.30 41 42
Previous studies across multiple countries and settings have demonstrated a positive relationship between vaccine confidence measured by VCI score and vaccine uptake. In our population VCI scores did not correlate with COVID-19 vaccine receipt, but did vary by healthcare worker role. The VCI may not capture attitudes specific to COVID-19 vaccination.17
A strong physician recommendation in favour of vaccination has been shown to positively influence vaccine decision-making for many immunisations, and COVID-19 appears no different.43 44 In our study, healthcare workers reported their primary care doctor was the most trusted source for advice on COVID-19 vaccination and this held true across race and vaccine receipt. Similar to other studies in the USA, black participants reported lower levels of trust in government agencies, highlighting the need to build trust and use trusted messengers in communities of colour.41 42 A study of healthcare workers in Canada also found that COVID-19 vaccine refusers were more likely to mention lack of trust in experts and pharmaceutical companies.25
Our findings also point to the influence that all healthcare workers can have in discussing COVID-19 vaccination within their social networks. Over 70% of the participants were asked about COVID-19 vaccination multiple times by coworkers, family and community members, adding evidence to support implementation of strategies that leverage healthcare workers as trusted messengers.45
Limitations
The high rate of COVID-19 vaccine acceptance in our population may be the result of response bias, where healthcare workers with favourable vaccine attitudes were more likely to complete the survey. As of July 2021, New York City hospitals reported 70% of workers have been fully vaccinated.46 Our study may have some limits in generalisability given the setting in New York City and a substantial representation from an academic health system.45–47 Additionally, black and Hispanic respondents were under-represented in our survey, comprising 10% and 16% of our survey population, respectively, whereas approximately 20% of the healthcare workers in our systems’ hospitals identify as black and 18% identify as Hispanic. While we cannot generalise to other parts of the healthcare system, such as long-term care facilities, we do think our results may be relevant to healthcare workers in a variety of settings.
We chose to use receipt as the primary outcome, rather than intent. As such, participants who indicated they ‘planned’ to receive the vaccine were categorised for the primary outcome along with those who stated that they did not plan to. We did review the differences between these two groups and assessed differences over time (see online supplemental file 9). Additionally, while the COVID-19 vaccines were made available to employees at the time of the survey, many may have had access issues, which our survey was not designed to assess. The 11% of respondents in our survey who reported they planned to get the vaccine but had not scheduled or gone for their vaccine yet may have experienced access issues. We recognise that access plays an important role in vaccine uptake, but to minimise length we did not include these measures in our survey. Future studies should investigate inequities in access to vaccines and to accurate information. Intervention design targeting marginalised groups of healthcare workers and others will need to account for the dynamic interplay between vaccine access and ease of access, respectful service delivery and vaccine behaviours.
Supplemental material
Conclusion
In this study of 1933 healthcare workers during the initial COVID-19 vaccine roll-out in New York City, the data demonstrated high overall receipt and confidence. Beliefs in the COVID-19 vaccine’s importance in protecting others were the strongest independent predictors of vaccine receipt. Even among healthcare workers with concerns about safety, side effects or being experimented on, over 50% did receive the first dose of vaccine, suggesting a potential pathway for intervention among these workers.
Our study demonstrated striking inequities in COVID-19 vaccine receipt. Black healthcare workers, adjusting for occupation and other factors, were less likely to receive the COVID-19 vaccine. A quarter of healthcare workers expressed concerns about being experimented on, particularly among marginalised groups. Addressing mistrust in public health and healthcare related to systemic racism will be critical to achieving a more equitable vaccine response.
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Anonymous data are publicly available on Open Science Framework (OSF) data repository with the persistent URL: https://osf.io/mhnrp/.
Ethics statements
Patient consent for publication
Ethics approval
This study received exemption determination from the Institutional Review Board at the Icahn School of Medicine at Mount Sinai (#20-01964).
Acknowledgments
We would like to acknowledge all the anonymous healthcare employees who took part in our survey and thank them for their care, strength and commitment during this difficult pandemic. We would also like to thank the COVID-19 Research Unit at Elmhurst Hospital (CURE-19), along with its sponsors, the Global Health Institute at NYC Health and Hospitals/Elmhurst Hospital Center and the Arnhold Institute for Global Health at the Icahn School of Medicine at Mount Sinai.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @nschwalbe, @duncanmaru
Contributors ABo, AF, AG, AH, CH, JJ, JK, SL, DM, SM, JM, KO, SP, DP, AF, ARo, LS, JL and RV conceptualised the study. ABa, ABo, NJD, CG, CH, JK, SL, DM, KO, NRS and LS developed the methodology. ABo, CH, JJ, DM, SM, KO, SP, ARa, NRS and LS developed the survey design. AH, JK, SL, DM, SP, NRS, LS, NV, NI and SR conducted dissemination. DD'S, CH, SP, ARa, LS, JL and RV curated the data. IN, SP and NV conducted data validation. AC, JK, RM, DM, JM, SP, ARa, NRS and LS analysed the data. DM and ARa created data visualisations. AC, AG, DM, KO, ARa and LS were responsible for project administration. KO, DM, AF, CH, LS, AH and NI wrote the original draft. SR interpreted additional data and wrote revisions for revised manuscript. All authors reviewed and edited the manuscript, provided relevant intellectual input, and read and approved the final manuscript. KO and DM have primary responsibility for the final content. KO will act as guarantor. The corresponding author attests that all listed authors meet the authorship criteria.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.