Article Text

Abstract
Objective The purpose of this study was to assess knowledge of and barriers to osteopathic medicine in Chinese immigrant communities in New York City (NYC).
Design A cross-sectional study was designed in which a culturally appropriate survey in Chinese and English versions was administered anonymously to measure immigrant perceptions and knowledge of osteopathic medicine.
Setting Data collection occurred in the municipal delineations for the Chinatown neighbourhood within the New York, New York borough of Manhattan.
Participants Community members were selected using convenience sampling from high-density areas to participate. Information gathered from the survey included demographics, education level, healthcare habits and knowledge of the osteopathic profession.
Results 120 surveys were conducted with 68 males and 52 females, with an average age=40. Respondents in the age range of 18–29 years, those with fluent English-language proficiency, and participants with graduate-level education status demonstrated a higher proportion of knowledge of osteopathic manipulative medicine and osteopathic physicians (doctors of osteopathic medicine) among the study variables.
Conclusion Compared with research on the general US population, a general lack of knowledge of osteopathic medicine exists within NYC’s Chinese immigrant community. Although this difference may be ascribed to linguistics and ethnosociological factors, greater outreach and education is needed in urban minority communities to make immigrants aware of all healthcare resources available during the current shortage of US primary care physicians.
- attitude to health
- community-based participatory research
- community medicine
- family health
- health communication
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- attitude to health
- community-based participatory research
- community medicine
- family health
- health communication
Key points
This article contributes valuable viewpoints towards public health by addressing healthcare disparity issues related to immigrant communities.
The findings suggest improvements that can be made in the effectiveness and efficiency of public health interventions to better primary care and overall health outcomes for immigrant populations by providing culturally appropriate health education and outreach.
Awareness and knowledge of osteopathic physicians and medicine has steadily grown since the inception of osteopathic medicine, resulting in increasingly positive attitudes and perceptions of the field. However, limited research exists on awareness and knowledge of osteopathic physicians and medicine within immigrant populations.
This research broadens previous studies on osteopathic awareness by the design of a culturally appropriate survey that can be translated and used in the Chinese, and by extension, other immigrant communities in the USA.
The conclusions of this study identify potential barriers in healthcare outreach in the Chinese immigrant community and other minority groups.
Introduction
From its inception in the late 19th century, osteopathic medicine (OM) has attracted a wide base of patients who appreciate OM’s holistic, interconnected, whole-body approach to medicine.1 2 International recognition of the osteopathic profession and its treatment modalities, including osteopathic manipulative medicine (OMM), have been relatively limited, despite varying degrees of practice privileges in over 50 countries.2–6 With allopathic physicians with doctor of medicine (MD) degrees serving as the primary healthcare providers in their native countries, many immigrant communities may have never been exposed to an osteopathic physician, or doctor of OM (DO), prior to re-establishing healthcare in America.3 5 7 In turn, this may have led to underutilisation due to unfamiliarity or even distrust. Recent clinical case reports highlight the advantage of OMM as a diagnostic and treatment modality.8 9 DOs are trained at colleges of OM, many of which are committed to training primary care physicians and addressing community health needs.10 Lack of awareness or knowledge of the osteopathic profession, thus, acts as a barrier to accessing healthcare, especially those in need of primary care physicians in underserved locations.11
Previous studies on osteopathic awareness in the USA have poorly represented minority communities, with minimal data looking at the perception and knowledge of the profession within those communities.12–17 This study aims to investigate osteopathic awareness by assessing the familiarity of DOs and OMM in one of the nation’s largest Chinese population—Manhattan, New York City, New York’s Chinatown. We hypothesise that greater osteopathic outreach and education needs to occur in Chinese communities to increase their access to primary care providers. This project also provides a framework for future research in other minority communities and characterises potential barriers that may hinder their access to OM and, by extension, overall healthcare.18
Methods
Participants
According to the 2010 US Census, the number one ranked city in the USA with the highest number of Asian Americans, over 1.1 million, is New York, New York.19 Participants were located in the municipal delineations for the Chinatown neighbourhood within the New York City borough of Manhattan.
Participants were informed, both verbally and with the inclusion of a cover letter, that participation was voluntary and responses required no identifiers to protect the anonymity of participants. Minors, those who did not demonstrate complete understanding of the basis of the survey, and those who were unable to give informed consent were omitted from this study.
Measures
A 12-question mixed multiple-choice and dichotomous (yes/no) survey was developed specifically for this study to measure osteopathic awareness. The survey was provided on paper in English and traditional Chinese (figure 1). The survey included questions regarding demographics (age, gender, education level), language (primary language, English proficiency), healthcare habits (regularity of doctor visits, type of doctors visited), knowledge of OM, and a clinical scenario of low back pain (LBP), one of the most common reasons for doctor visits and one for which osteopathic manipulative treatment has been shown to effectively treat, was provided to participants.20–25
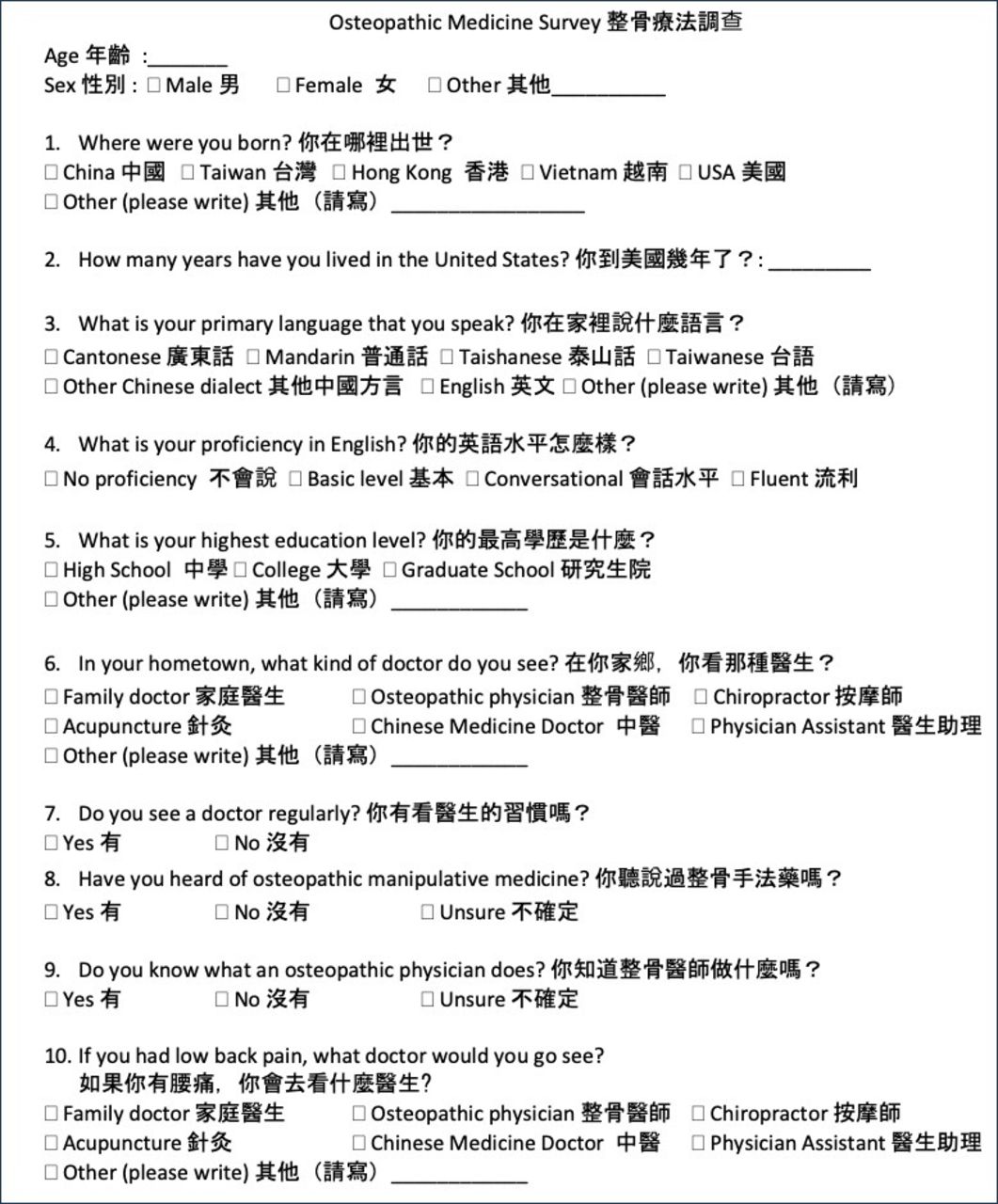
Survey in English and translated into traditional Chinese.
Data collection
Medical student researchers were located within the municipal delineations for the Chinatown neighbourhood within the New York, New York borough of Manhattan and used convenience sampling in high-density areas, including major thoroughfares and parks (figure 2), to obtain participants available for the study. No inclusion criteria were identified prior to subject selection. All subjects were invited to participate. No other specific recruitment methodologies were used. No financial compensation or other incentive was provided to participants who voluntarily took the survey. Collection occurred over four consecutive days, Thursday, 13 July to Sunday, 16 July 2018.

{kind=link}
{kind=link}
High-density areas in Manhattan’s Chinatown were selected for the desired population as delineated by the blue lines. Participants were randomly surveyed with a paper survey in an anonymous fashion.
Data analysis
Survey data were scanned, and a data spreadsheet was electronically created using a licensed version of Microsoft Excel, V.2016 (Microsoft Corporation, Redmond, Washington, USA). The data were subsequently coded for statistical analysis. Group comparisons were completed using Pearson’s χ2 tests of independence to examine the difference, if any, between health habits and demographics (age, sex, birth location, years in the USA, primary language, English proficiency,education level) and awareness of the DO profession and knowledge of OMM. Statistical analysis was performed using the release version R-2.15.3.tar.gz of R: A Language and Environment for Statistical Computing, developed in Vienna, Austria by the Core Team of the Foundation for Statistical Computing.26
Results
A total of 120 participants were surveyed and included on analyses of participant demographics versus familiarity with DOs and OMM. A total of 68 males and 52 females were included in the study, with an age range of 18–80 and a mean age of 40±10.56. Of the 120 participants surveyed, only 16% (n=19) indicated knowledge about OMM, and 15% (n=18) indicated knowledge of DOs, with demographics generally similar to the overall community. Detailed demographic data and results are displayed in table 1).
Demographic characteristics of all participants compared with participants with knowledge of DOs and OMM
In this study, knowledge of DOs was highest among Chinese groups who were young, proficient in the English language, and held a college degree. Concerning age, knowledge of DOs was significantly higher among the youngest age group investigated (18–29 years old), where 44% of the participants reported having knowledge of DOs compared with other age groups (22% and lower, p<0.044, table 1). Additionally, knowledge of DOs was significantly higher for participants with English proficiency compared with non-English speakers (94% vs 6%, p<0.035). Concerning education, 44% of the participants with a college degree reported having knowledge of DOs compared with lower levels of education (p<0.03), where only 28% of participants with a high school degree reported knowledge of DOs). Among the Chinese immigrants surveyed, no significant differences in knowledge of DOs and OMM were found among groups that varied on location of birth, number of years living in the USA, and primary language (table 1).
Concerning healthcare habits of the study participants, no difference in knowledge of DOs or OMM was found between those who visited their doctor regularly versus those who did not see their doctor regularly (table 2). Of those participants who do see their doctor regularly, 78% reported seeing their family physician (table 2). Concerning the clinical scenario of low back pain (LBP) that was presented to study participants, although 49% of the participants reported they would see their family physician and 24% would see a chiropractor, no participants indicated that they would see a DO (table 2).
Health habits of participants versus those with knowledge of DOs and OMM
Discussion
A general lack of awareness of DOs and OMM exists within the Chinese community in New York City’s Manhattan Chinatown. Survey participants did not recognise the osteopathic profession, especially among the elderly. Statistically significant factors contributing to this lack of knowledge include age, English proficiency and education. Compared with similar studies in the past, this study found the gap in minority osteopathic familiarity even greater than previously noted, with less than one in five participants indicating knowledge of OM.17 In the decennial OSTEOSURV 1998, 2000 and 2010, Asians are presumably included in the category of ‘other (including >1 race)’ and ‘non-Hispanic’, leading to a gross simplification and lack of targeted data for the Asian population in America.3 12 15–17 Current research has also focused primarily on osteopathic recognition in European settings, with minimal attention in Asian communities based in Asia or the USA.27 28 Numerous studies have validated the need for disaggregated data as a way of dissecting health trends and practices within Asian communities.13 14 29 While this study was unable to definitively determine a sole cause, exploring the numerous factors such as linguistics and history can provide some context for lack of osteopathic awareness and potential barriers to outreach.
Age (18–29), English-language proficiency (self-identified fluency) and education level (college graduate) were statistically significant in exploring whether the participants had knowledge of DOs and OMM. Adults younger than the age of 30 demonstrated a statistically significant relation with knowledge of what an osteopathic physician does in comparison to adults older than the age of 60, contrary to previous research done that imply the opposite.24 With an ever-increasing number of osteopathic physicians entering the workforce coupled with shifting trends in healthcare consumption, the under 30 age demographic can be a future area of expansion for the OM profession as this generation straddles the divide between separation and assimilation in broader models of acculturation.15 25 27 English language proficiency additionally demonstrated a statistically significant relation with knowledge of what a DO does in comparison to adults without English language proficiency due to the linguistic and historical nuances that separate and unite allopathic and OM.27 28 Unsurprisingly, to coincide with English language proficiency, educational status, particularly those having a college degree, also showed statistical significance in knowledge of DOs and OMM, compared with adults without a college degree, which is a common socioeconomic factor that correlates with higher health literacy and self-advocacy to explore alternative options such as DOs and OMM.14 29 Despite the lack of statistical significance in other demographic categories on DO and OMM knowledge, it is important to acknowledge their potential influence and impact in patient knowledge and choice.
Under the auspices of A.T. Still MD, DO, OM was founded in 1874 as an alternative to allopathic medicine.1 In the same time period, modern medicine, commonly referred to as ‘Western’ medicine, arrived in China at the end of the 19th century after its defeat in the Opium Wars.30 Backed with interventional therapies and single drug pharmaceuticals, modern medicine supplanted more conservative traditional remedies and healers.31 With modernisation of medicine, semantic genericization of medical classifications and terms resulted in an inability to capture the difference between osteopathic and allopathic medicine.30 31 For example, in the Chinese spoken dialects and unified written system, there are no characters or conventions for describing OM vis-à-vis allopathic medicine. On presentation to a patient, an osteopathic physician would identify themselves as yi-sheng (醫生), which is exactly how an allopathic physician would identify. When translating the term ‘osteopathic’, numerous sources use gu-ke (骨科) which means ‘of, or relating to the study of bones’, which can be confusing and misleading as orthopaedics and other bone specialties use the same term. A viable solution could be the use of zheng-gu (整骨) for osteopathic, which when translated, means ‘whole-bone’ and is more representative of the its meaning. In order for the community to adopt this, however, it would require more outreach to transition to common vernacular.
A conceivable challenge to awareness is the lack of osteopathic medical schools in Asia.32 Osteopathic medical schools are predominantly located in the USA, with physicians graduating with full practice rights in relation to their allopathic counterparts. Conversely, in non-American osteopathic medical schools, graduates are osteopaths, who solely perform OMM.3 33 This dichotomy complicates perception of OM, as demonstrated in international licensure. A prime example is seen in Taiwan, in which their licensing board translates ‘osteopathic physician’ as ‘bone doctor’, which is the same as a chiropractor. In an effort to educate the international community regarding the capabilities of American-trained osteopathic physicians, numerous initiatives have been started, ranging from partnerships between osteopathic medical schools and hospitals in Asia to the International Primary Care Educational Alliance’s China Project, which trains physicians in China on osteopathic family medicine.34–36 International licensure and practice rights continue to be a priority for the American Osteopathic Association, leading to partnerships with the Osteopathic International Alliance and the Bureau of International Osteopathic Medicine, and resulting in recognition by the United Nations and increased practice rights in countries such as South Korea.3 37
This multilayered approach and contextual/nuanced view are needed if osteopathic awareness is to occur in Asian, and by extension, ethnic minority communities that lack exposure to the field. In this study, those who had no knowledge of OM would not see a DO for LBP relief and while most participants would see their primary care doctor/family care doctor, this does not preclude the possibility of that physician also being an osteopathic physician. For example, there are several osteopathic physicians at the Charles B. Wang Community Health Center, which is based in the heart of Manhattan’s Chinatown. It is conceivable that some of the participants have an osteopathic physician as their primary care doctor, but do not distinguish between the two entities.38–40 The lack of differentiation compounded by whether or not the osteopathic physician decides to practice OMM at patient visits may result in the possibility of clinical care that is indistinguishable from allopathic physicians. Furthermore, participants also indicated they would see a chiropractor for their LBP. Due to the historical roots of chiropractic, many of the techniques share similar mechanisms to OMM.41–43 Coupled with similar nomenclature in the Chinese language, future studies could assess the effectiveness of OMM demonstrations/pamphlets on the willingness to see a DO.
With the broad implications on osteopathic awareness in the Chinese community, there are several limitations in this study. Manhattan’s Chinatown is but one of several high-density areas for the Chinese community in New York City, which may not be a true representation of osteopathic awareness in the large community. Furthermore, surveys were conducted midday which may fail to capture Chinese community members that are working or not in the area. It was also difficult to assess whether age and osteopathic awareness trends were skewed by immigration status, as almost all participants over the age of 60 had immigrated to America. This could suggest a correlation between lack of osteopathic awareness and immigration status, further affirming that many immigrant minority communities have little to no exposure to OMM and DOs. Future studies may explore the relationship between immigration status and osteopathic awareness, comparing multiple Chinese communities across New York City at varying times of day, or comparing osteopathic awareness across other Asian communities with a qualitative or mixed-method study.44 45
Conclusion
There is a general lack of awareness of the osteopathic physicians and OMM in the Chinese community in New York’s Manhattan Chinatown. Regardless of age, gender, country of origin, English proficiency or level of education, participants did not recognise the profession, which may be a reflection of the lack of outreach in ethnic minority communities. Despite proven efficacy of OMM on LBP, the Chinese community does not know that OMM is a suitable option for conservative management. This study may attract more researchers to design a framework for assessing other ethnic minority communities and their knowledge of the osteopathic field.
References
Footnotes
Twitter @clomiguenmd
Contributors JC, SL, GY, YAZ, PJW, ED, MV, SS, MAT and CML equally: provided substantial contributions to conception and design, acquisition of data or analysis and interpretation of data, drafted the article or revised it critically for important intellectual content, gave final approval of the version of the article to be published, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Touro College Health Sciences Institutional Review Board for the Protection of Human Subjects (HSIRB #1777).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplementary information. Data are available on reasonable request to the corresponding author.