Article Text

Abstract
Introduction The International Family Medicine Clinic (IFMC) was established in 2002 by the University of Virginia Department of Family Medicine to provide comprehensive, timely, culturally sensitive and high-quality healthcare to the growing refugee and special immigrant population in Central Virginia, USA.
Methods The purpose of this paper is to describe the IFMC, with a specific focus on interprofessional roles, interprofessional collaboration, community partnerships and the services and resources available to IFMC patients.
Results The clinic has served over 3100 refugees from 60 countries in its 16-year history. In 2019, the clinic staff now includes 4 attending physicians, 2 nurse practitioners and 14 residents who have dedicated clinic time to see refugees; a registered nurse care coordinator and a social worker dedicated to the IFMC refugee population; 2 clinical psychologists and doctoral students in clinical psychology; and a clinical pharmacist. The IFMC also provides onsite psychiatric care. A process flow map depicts the interconnectivity of interprofessional team members working together with other specialty care providers within the medical centre and with community partners on behalf of refugee patients through the resettlement process.
Conclusion Individuals who arrive in the USA as refugees are a particularly vulnerable patient group and often require an interprofessional team approach. The IFMC may serve as a model for other institutions interested in starting a similar interprofessional, refugee-centred medical home.
- refugees
- immigrants
- interprofessional team
- primary healthcare
- patient centered medical home
- model of care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- refugees
- immigrants
- interprofessional team
- primary healthcare
- patient centered medical home
- model of care
Introduction
Refugees are a special type of foreign-born resident of the USA; the term refers to a temporary legal status defined by the United Nations High Commissioner for Refugees as any person who has been forced to flee his or her country because of persecution, war or violence for reasons of race, religion, nationality, political opinion or membership in a particular social group.1 Since 1975, the USA has resettled more than 3 million refugees and historically has welcomed more refugees than other countries globally.2 Individuals who hold Special Immigrant Visas (SIVs)—since 2006 a programme for certain Afghan and Iraqi nationals—receive the same federal resettlement support in the USA.3
With regard to medical care, the USA has well established clinical guidelines for providing primary care4 and expert guidance focusing on practice management issues in the provision of care for refugees.5–7 In addition, refugee and healthcare provider perspectives on receiving and providing primary care in countries of resettlement highlight challenges in accessing care, understanding new healthcare systems, the importance of trusting patient-provider relationships and the value of culturally competent care.8–10 Studies, including two published about the International Family Medicine Clinic (IFMC), show outcome measures that demonstrate how models of care dedicated to refugee populations can improve quality of care by decreasing wait times to initial visits,11 12 decreasing inappropriate emergency room visits,13 14 improving management of chronic diseases15 and decreasing the need for specialty referrals by having primary care providers (PCPs) who are trained in the unique medical needs of refugees.12 There are a few published examples of refugee centred collaborative models and medical homes across the USA and Canada,16 17 as well as papers written by experts who have advocated the importance of providing comprehensive, interprofessional care to refugee patient populations.18 In addition to language barriers, the care of refugee patients is often complicated by cultural differences, lack of previous health records, social barriers and complex psychosocial histories. Therefore, a multifaceted, interprofessional approach to providing comprehensive care is necessary. In this paper, we add to what is known by focusing on interprofessional roles inside a refugee-centred medical home and by providing specific details about how individuals in these roles operate collaboratively both within the IFMC and with external partners.
Background
IFMC was established in 2002 by the University of Virginia (UVA) Department of Family Medicine to provide comprehensive, timely, culturally sensitive and high-quality healthcare to the growing refugee population in Central Virginia, USA. Through an informal agreement with the local resettlement agency (RA), the IFMC provides a medical home to all refugee and SIV newcomers (hereafter called refugees) who resettle in Charlottesville and are supported by the USA federal resettlement programme. The clinic has served over 3100 refugees from 60 countries in its 16 year history (table 1).
Characteristics of patients seen in the IFMC 2002–April 2019 (n=3181)
For children under 18, the most common diagnoses are well child and other medical examinations/evaluations; immunisations and screening for infectious diseases; anaemia and other nutritional endocrine and metabolic disorders; upper respiratory infections; allergies; disorders of the teeth and jaw; gastrointestinal disorders; genitourinary symptoms; skin disorders; and developmental conditions. For adults, the most common diagnoses are medical examinations/evaluations; immunisations and screening for infectious diseases; hypertension; back problems; lipid disorders; other connective tissue disorders; skin disorders; headaches including migraines; diabetes mellitus; and mood disorders.
The IFMC is located within the Family Medicine Clinic (FMC), a National Committee for Quality Assurance (NCQA) Patient Centered Medical Home (PCMH) accredited practice, on the main campus of the University of Virginia Health System. There is no special funding for the clinic as it operates within the FMC, using the same facilities, reception and nursing staff as for other patients. IFMC patients are billed through their insurance, including Refugee Medical Assistance (available for refugees for the first 8 months after arrival),19 Medicaid, Medicare, or are given discounted or no cost care if they qualify through a state financial assistance programme.
Of the 59 languages (excluding English) represented by patients who attend the IFMC, clinic staff have access to telephonic, video and in-person interpreters for all but two of the languages. Since the majority (71.8%) of individuals who attend the IFMC do not speak English on arrival and many never learn English to the extent to which a meaningful clinic visit could be conducted by an English-speaking healthcare provider, interpreters are used for most office visits.
History and evolution of professional roles in the IFMC
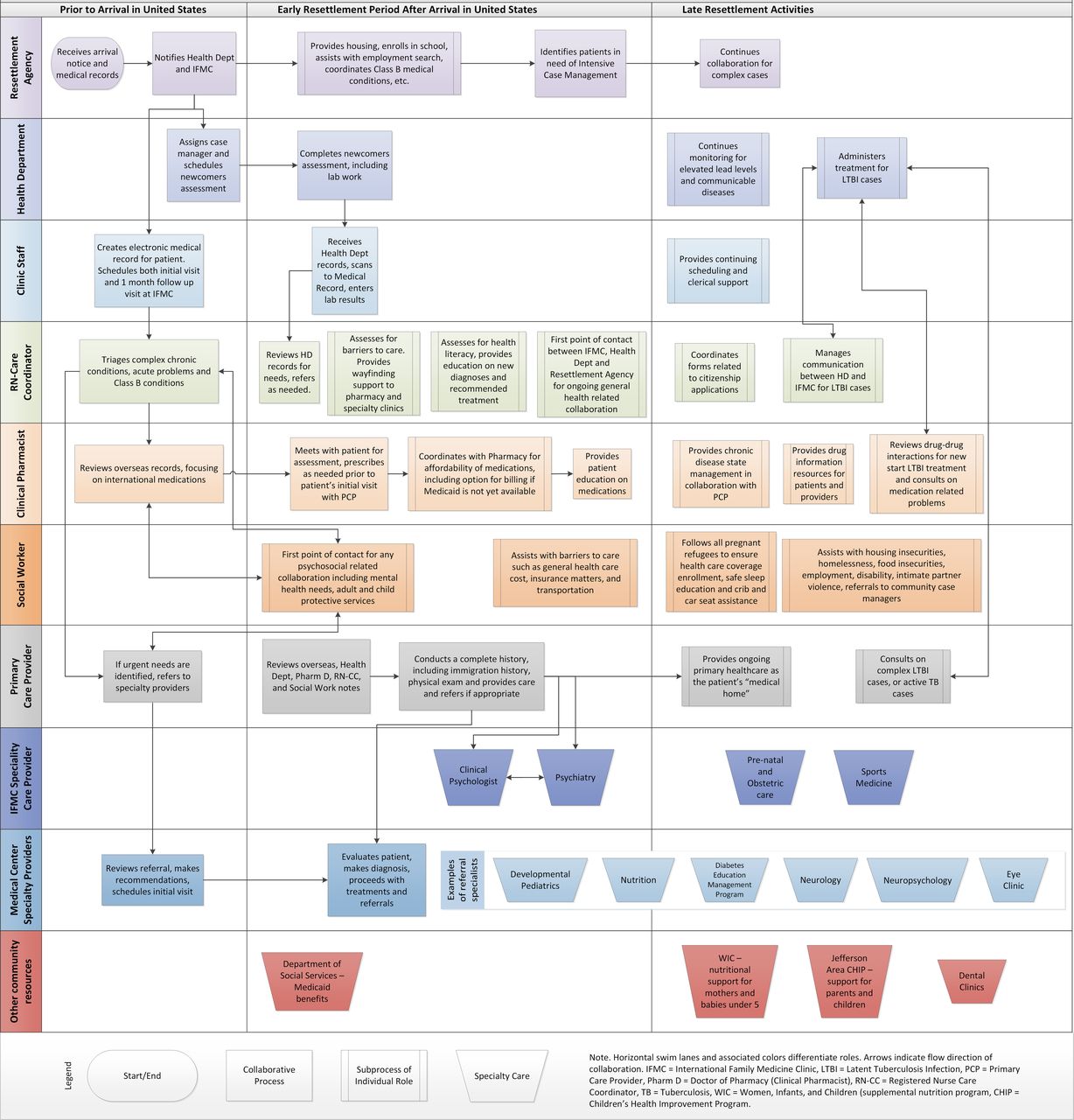
Since inception in 2002, the clinic’s staff has grown to include physician faculty, resident physicians and nurse practitioners and also a strong core of interdisciplinary professionals who collaborate to provide comprehensive care to refugees. In 2019, it now includes 4 attending physicians, 2 nurse practitioners and 14 residents who have dedicated clinic time to see refugees; a registered nurse care coordinator (RN-CC) and a social worker (SW) dedicated to the IFMC refugee population; 2 clinical psychologists and doctoral students in clinical psychology; and a clinical pharmacist integrated into the IFMC as part of the role in the FMC. The IFMC also provides onsite psychiatric care through the UVA Department of Psychiatry. The process flow map for the IFMC and its external partners that is provided in figure 1 demonstrates the interconnectivity of team members working together on behalf of the patients during their resettlement process.

{kind=link}
Process flow map illustrating interagency and interprofessional collaboration for healthcare for newly arrived refugee.
Description of specific roles
Registered nurse care coordinator
The RN-CC is the first point of contact for nearly all refugees who have a special medical need that is known prior to their arrival in Charlottesville. Class B medical conditions, identified in the overseas medical screening, are those that do not preclude the individual from travelling to the USA, but represent a departure from normal health and require timely follow-up after arrival.20 Over the past five fiscal years (2013–2018), 19% of new patients to the IFMC had one or more Class B conditions (see table 2). Examples of Class B conditions in adults include dialysis dependent chronic kidney disease, untreated Hepatitis C, liver cancer, asthma, hypothyroidism, back pain, blindness, migraine, chronic obstructive pulmonary disease, hypertension and cardiomegaly. Recent cases involving children included those with physical or developmental disabilities, genetic abnormalities and congenital heart defects. The RN-CC is contacted in advance by the medical case manager of the RA and then secures an expedited appointment to establish care in the IFMC, and in some cases obtains an early referral from an IFMC provider to a specialty provider when needs are urgent. When profound medical conditions are indicated on the overseas medical screening the RN-CC consults with the assigned PCP and works to schedule specialty appointments immediately after and sometimes even before the Initial Visit at the IFMC. For individuals holding SIVs, overseas medical reports are not received in advance, so any urgent medical conditions are addressed after arrival in the USA. Initial visits for refugees without urgent needs are scheduled by the front desk staff, typically 8 weeks after arrival in the USA.
Total number of new patients* and known Class B conditions ( ≥ 1) for refugees by fiscal year
Class B conditions identified at the overseas medical screening often do not fully capture the scope of health needs at arrival. Other ways patients are identified as needing care coordination before the first visit include:
The RA may learn of medical issues during the home visit made 24 hours after arrival or days to weeks later when people return for cultural orientation or English classes.
The health department (HD) performs a health screening within 45 days of arrival,21 which includes screening for communicable diseases as well as selected chronic diseases in adults as required by the Centers for Disease Control and Prevention (eg, hypertension, high cholesterol, diabetes) and special screenings for children (especially those required for school enrolment like vision and hearing, lead levels and complete blood count).4 22 When the HD identifies a health problem, they contact the RN-CC to coordinate follow-up.
Patients may have an urgent or emergent need before their initial clinic visit and go directly to the emergency department (ED) or a walk-in clinic. Recent examples of ED visits before initial intake include leg abscess, URI, pregnancy symptoms, impetigo and metabolic acidosis with dehydration. Workers at the RA are often aware of these visits and alert the RN-CC to coordinate follow-up.
At this stage, the IFMC RN-CC and clinical pharmacist sometimes collaborate to arrange for care that will bridge a person to their initial visit at the IFMC; for example, if the patient has a known chronic problem and simply needs a medication refill. Table 3 presents a summary of the care coordination needs for refugees over a recent 18-month period.
Summary of cases (n=78, 37% of 210 total new patients) requiring RN care coordination before or directly after initial IFMC visit during the 18-month period from 1 September 2017 to 28 February 2019
The RN-CC plays an important role in helping to orient newly arrived individuals and families to the USA healthcare system, including teaching them how to schedule follow-up appointments; to expect phone calls from the clinic about test results and any subsequent recommendations; to navigate to pharmacies or specialty clinics; and to request an interpreter if one is not immediately offered. This orientation includes explaining conventions unique to the USA healthcare system such as the fact that patients are routinely asked to identify themselves by name and date of birth and that they need to memorise their legal date of birth even if that date has never held relevance for them before.
Once patients have established care at the IFMC, the RN-CC continues to assist those with any chronic or acute illness for as long as there is a need, no matter how long they have been living in the USA. For example, patients with anaemia, elevated lead levels or infections are provided treatment support (eg, teaching a patient with Helicobacter pylori how to take triple therapy appropriately) or monitoring by the RN-CC until the acute issue is resolved or improves. Patients with chronic illness may see the RN-CC to support their understanding of the condition and long-term medication regimens, to refill monthly medication boxes, and for coaching and support on lifestyle modifications such as improving their nutritional habits. The RN-CC also collaborates with the HD to aid in the care of patients with latent and active tuberculosis infection to ensure appropriate treatment, follow-up and documentation in the electronic medical record. These are examples of how the RN-CC’s role in both external and internal interprofessional collaborations has improved the quality of care for patients in the IFMC. Future work will seek to quantify how these efforts have impacted quality measures.
Transitional Care Management in the clinic involves reviewing cases of all patients who have been admitted to the hospital to identify gaps in care and reduce readmissions. The refugee patients benefit from this resource as well, as the RN-CC calls all who have been discharged within 2 days to assess symptoms and review medication adherence.
The RN-CC is often the first point of contact with outside agencies that also work with these families. For example, individuals working with the school system; a nurse home visit programme—called CHiP—serving low-income families with young children; Women, Infants and Children (WIC); or English as a Second Language programme will alert the RN-CC to problems or barriers that families experience. The RN-CC will work with the family and their social supports to build trust and optimise their care in a way that suits the family best.
Social worker
The IFMC SW assists with: overcoming barriers to healthcare via referrals for health insurance, Medicaid and UVA’s billing and prescription discounts; housing insecurity and homelessness; employment resources and vocational rehabilitation; school matters; food insecurity; intimate partner violence; adult and child protective service concerns; disability guidance; accessing dental care and accessing longer-term mental health and substance abuse treatment. With patient consent, the SW collaborates with community partners including the refugee RA, CHiP and the Department of Social Services. The SW follows all pregnant women to ensure healthcare coverage, provides safe sleep education, assists with crib and infant safety seat applications through the HD and refers to WIC. The SW connects ageing patients and their families with senior centres, adult day care and in-home caregiver resources. The SW is available for crisis and supportive counselling. In addition, the SW assists patients and families with discussion of end of life planning as well as advance medical directives. The SW also collaborates with the team to refer patients to hospice care and works closely with UVA’s Palliative Service as well as hospice agencies when needed.
Clinical pharmacist
Clinical pharmacists enhance the quality of care provided in the primary care setting.23 Carter et al 24 demonstrated that latent tuberculosis completion rates were improved by incorporating the clinical pharmacist as part of the care team, assisting with medication education and management. Within the IFMC, the clinical pharmacist, who holds a Doctor of Pharmacy (PharmD) degree, is actively involved in the clinical care of many refugee patients. The PharmD provides support to the PCP to assist with chronic disease state management while working under a collaborative practice agreement, provides education and ensures access to medications and serves as a resource to clinical staff for medication-related issues. Since the role of the PharmD was first introduced to the FMC as a whole in 2015, it has evolved over time to encompass changing patient care demands specific to the IFMC, to include additional disease state management and assistance with overseas medications with new arrival patients. For new arrivals, the clinical pharmacist reviews overseas medical records and often meets with the patient prior to their PCP visit to ensure the patient has access to medications on arrival. The PharmD can also spend an extended amount of time reviewing medication regimens to provide education, ensure access and assist with alleviating cost burdens. A recent study of PharmD interventions in the IFMC demonstrated a reduction in A1c levels for referred refugee patients with diabetes.15 The average time spent for each encounter with refugee patients by the PharmD was 30.1 min with a range of 5–90 min. In their work with the IFMC, the RN-CC, SW and PharmD are supported by the Health System’s Ambulatory Services, Department of Social Work and Department of Pharmacy, respectively.
Behavioural health
The IFMC includes integrated behavioural health (BH) services provided by clinical psychologists, psychiatrists and their trainees. This onsite integrated care model improves accessibility by avoiding navigation to other clinics and reducing the stigma surrounding mental health services. Additionally, providing mental health services within the clinic allows access to the hospital’s language interpretation services, which are generally not available in community mental health providers’ offices. Another advantage of the integrated care model is that it provides refugee patients, who are juggling many competing tasks, with mental health interventions in small (one or two sessions) doses, every few months. Being onsite in the IFMC allows the BH providers to coordinate with the other IFMC team members and stay in touch with the refugee patients’ evolving needs. Refugees are sometimes seen by the BH providers at the same visit when they see the IFMC physicians or other team members and are often introduced to the BH providers by the already-known team member. This helps alleviate some patients’ anxiety about seeing a mental health provider, which has often carried an even larger stigma in their home country. Referrals are made by IFMC PCPs directly to the IFMC psychiatry team when needed; the latter see patients weekly onsite in the Family Medicine clinic. Alternatively, patients can schedule BH visits at the clinic front desk or by calling the clinic. Non-English speakers can call and leave their name and language, and the clinic calls them back with an interpreter.
The BH providers address trauma and adjustment disorders common to refugees as well as mental health issues of a more general nature such as symptoms of mood and anxiety and substance use disorders through individual, couple or family sessions. Brief interventions as well as longer-term psychotherapy and medication management are offered. Family and individual therapy are available to children with behavioural or adjustment disorders and to families struggling with the challenge of raising adolescents in a new culture. Infants and toddlers are screened for developmental problems and autism at well-child visits. The BH clinicians use a range of evidence-based therapies depending on the patient’s needs, but all methods are grounded in a person-centred approach and build on the patient’s strengths.
Educational opportunities
The interprofessional design of the IFMC allows for a multitude of educational opportunities for students, residents and other learners. The duration and intensity of the training vary depending on the specific programme requirements. The opportunities for medical education start with shadowing opportunities for UVA undergraduate students; the IFMC receives many requests from students to learn more about refugee care as well as offers to volunteer. There is also a dedicated elective for fourth-year medical students, called ‘Caring for Refugees in Charlottesville’, during which the student sees refugee patients with a provider in clinic, rotates with the RA, the HD and the UVA travellers’ clinic and spends time with the RN-CC, SW and PharmD. By the end of the month, students have chosen their own research project and written a final paper addressing a relevant refugee health or culture topic, which are posted on the IFMC website.25 Research electives are also available to medical students and have resulted in peer-reviewed publications.26 27
Starting as interns, the UVA Family Medicine residents begin caring for refugees in the inpatient setting and for acute outpatient visits. A dedicated orientation is held annually to introduce the rising second-year residents to refugee care, as they will be caring for a panel of continuity patients in the outpatient setting. The residents have 1–4 half-days of clinic dedicated to refugee care per month and see refugees outside of these designated days. This direct longitudinal experience provides education in cultural competency and allows learners to gain and apply knowledge to their broader patient population. For each residency class, there is a dedicated workshop on refugee care focusing on increasingly complex topics. Additional opportunities are available for physician residents from other residency programmes; typically, 1–2 residents from Paediatrics or Internal Medicine will rotate through a dedicated refugee clinic elective per academic year.
Direct care for refugees is an important curricular component for the doctoral candidates in clinical psychology as well, who are an essential part of the integrated care team. Pharmacy students and residents, nurse practitioner and registered nursing students, and social work students also have gained experience in refugee care. Each Family Medicine faculty member has an opportunity to see and precept refugee patients. There are opportunities for faculty development and continuing medical education through attendance at national and international educational conferences.
Monthly international grand rounds bring speakers, both local and international, to share their invaluable perspectives, knowledge and experience working with refugees with the Family Medicine department. Topics range the gamut from specific diseases and mental health conditions (eg, thyroid disorders, dermatological conditions, parasites, tuberculosis, depression, post-traumatic stress disorder (PTSD), to cultural considerations (eg, views of end of life decisions among Bhutanese elders, reflections of a Canadian refugee care provider from her recently published book), to administrative updates (eg, federal refugee policies and anticipated arrivals, accessing social services, citizenship process).
The scope of research that has been done mirrors the evolution of the refugee population in Charlottesville, and members from each part of the IFMC team, including nurses, have been involved in quality improvement research aimed to improve the care of the refugee patients and the education of the providers who care for them. The IFMC maintains a database of its patients derived from the electronic medical record facilitating a variety of chart abstraction projects, for example, immunisation rates among refugee children,28 cervical cancer screening among refugee women,29 H. pylori screening and treatment, and lead screening among newly-arriving children.27 These projects have provided valuable information that has allowed the IFMC to identify gaps in care and implement improvements to better care for this population.
Key characteristics of the IFMC Interprofessional team
The IFMC interprofessional team has cultivated several key characteristics over time, reflecting themes found in publications on interprofessional collaboration.30–33 At a systems level, the team functions in an organisational environment that has created formal structures for interprofessional practice, including monthly IFMC resident meetings quarterly meetings with community partners, monthly clinic team and all-practice meetings and weekly hospital discharge meetings.30
Regular communication between team members allows for improved collaboration and support, whether that be through the above-mentioned regular communication channels or one-on-one discussions related to specific patient or family care needs. While the IFMC Medical Director will make operational decisions, team member input is valued and desired. Having the structure of a collaborative and supportive team also provides the opportunity for emotional support and recognition of some of the challenges that can come from serving this vulnerable and often challenging patient group. There is emphasis that providers need not try to solve all the patient’s issues and should instead reach out to other disciplines and team members within the clinic, health system or community for collaborative assistance. Finally, communication is not limited to only providers, community team members and clinical staff, but also includes a mechanism to engage patients in the overall clinical management and process. An IFMC patient serves on the department’s Patient Advisory Council, which is a panel of patients from each clinic site, thus ensuring that the refugee patient population is represented when clinical decisions and process changes are made or considered. The patients who arrive in Charlottesville as refugees benefit from the clinic’s PCMH endeavours, which include, but are not limited to, improved access to care and care management for chronic diseases.11
Case study
The following fictionalised example shows how the IFMC interprofessional collaborative model meets the challenging medical needs of many IFMC patients.
IFMC received notification from the RA of a new family arriving with SIVs from Afghanistan. The family was scheduled for Initial Visits allowing for 1 hour long appointments for each family member, clustered together in the same clinic session. Maryam (not her real name) is the 43-year-old mother of 4, who arrived with her husband and only three of her children. Her oldest child remains overseas in an unsafe area. Three weeks after their arrival, at her initial health screening at the HD, Maryam had elevated blood pressure and told the HD nurse she had run out of her medication. Her appointment to establish care at the IFMC was still 4 weeks away. The HD contacted the IFMC RN-CC who consulted with the PharmD and a medication appointment was scheduled for the next day. The RN-CC coordinated with the RA’s medical case manager, who provided transportation to the appointment since the family had not yet been to the clinic. The PharmD met with Maryam, reviewed and evaluated her medications from her home country and prescribed equivalent USA medications. Maryam was able to pick up her medications from the health system pharmacy and resumed taking them. For patients such as Maryam who need medications before their Refugee Medical Assistance health insurance is activated, UVA Pharmacy does not charge the patient or RA at that time. When the health insurance is activated, the pharmacy then bills the medication directly to the Refugee Medical Assistance health insurance, thus providing a service to the patients and avoiding billing mishaps.
A few weeks later Maryam had her initial visit with her PCP and the visit revealed good blood pressure control. In addition, she was showing signs of depression. She was seen by the Behavioral Health Team during her initial visit and again later for several follow-up appointments. The PCP also identified a need for dental care. The IFMC SW met with the patient during the visit and explained how to access adult dental care in the community. Maryam also had chronic headaches and knee and back pain which required treatment and follow-up appointments with her PCP. Future visits addressed new concerns and age-appropriate preventive care.
Conclusion
Interprofessional collaboration in primary care has been shown to benefit health systems and patients, particularly those with complex healthcare needs.30 Individuals who arrive in the USA as refugees are a particularly vulnerable patient group and often require this team approach.17 The case study illustrates the patient-centred, collaborative approach taken to improve care for all of the refugees who attend the IFMC. This paper provides specific detail about particular professional roles and the ways that these roles collaborate to improve care for refugee populations. For clinicians interested in initiating a similar model in other settings, a suggested first step is reaching out to local refugee RA(s), HDs and other organisations serving refugees, completing an assessment of community health needs and beginning discussions about interprofessional and interagency collaboration. By initially using available resources and existing staff, while ensuring access to language interpreters, interprofessional teams can grow to respond to the particular needs of their local refugee community. The authors hope that the IFMC may serve as a model for other institutions interested in starting a similar interprofessional, refugee-centred medical home.
Key points
In the setting of an academic medical centre’s Family Medicine clinic, this paper describes a 16-year history of interprofessional collaboration and community partnerships which have improved the timeliness and quality of care for individuals who resettle as refugees in a community in the USA.
A process flow map depicts specific tasks and activities by interprofessional healthcare provider role across the timeline of refugee resettlement; and a case study exemplifies collaborative work on behalf of this unique patient population.
Acknowledgments
We thank Kawai Tanabe, MPH and Amanda Sebring, BA for their assistance with the tables and figure.
References
Footnotes
Contributors We attest that all authors have made substantial contributions to the conception of the work, each participated in drafting the work and revising it critically for important intellectual content and had final approval of the version published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This article did not require institutional review board approval. According to the University of Virginia IRB-Human Subjects Research office, case studies may be published without IRB oversight, as long as they are redacted of all HIPAA identifiers. Our case study does not involve an identifiable living individual and contains no HIPPA identifiers.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.