Article Text

Abstract
This article illustrates quality improvement (QI) methodology using an example intended to improve chlamydia screening in women. QI projects in healthcare provide great opportunities to improve patient quality and safety in a real-world healthcare setting, yet many academic centres lack training programmes on how to conduct QI projects. The choice of chlamydia screening was based on the significant health burden chlamydia poses despite simple ways to screen and treat. At the University of Michigan, we implemented a multidepartment process to improve the chlamydia screening rates using the plan-do-check-act model. Steps to guide QI projects include the following: (1) assemble a motivated team of stakeholders and leaders; (2) identify the problem that is considered a high priority; (3) prepare for the project including support and resources; (4) set a goal and ways to evaluate outcomes; (5) identify the root cause(s) of the problem and prioritise based on impact and effort to address; (6) develop a countermeasure that addresses the selected root cause effectively; (7) pilot a small-scale project to assess for possible modifications; (8) large-scale roll-out including education on how to implement the project; and (9) assess and modify the process with a feedback mechanism. Using this nine-step process, chlamydia screening rates increased from 29% to 60%. QI projects differ from most clinical research projects by allowing clinicians to directly improve patients’ health while contributing to the medical science body. This may interest clinicians wishing to conduct relevant research that can be disseminated through academic channels.
- chlamydia screening
- quality improvement
- healthcare delivery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Introduction
Healthcare organisations continually strive to improve patient care services and quality through initiatives driven by their leadership and healthcare payers (eg, Centers for Medicare and Medicaid Services).1 Quality improvement (QI) projects in healthcare provide opportunities to advance best practices and enhance the redesign of healthcare to improve patient quality and safety.2 3
The modern study of QI has its origins in industry dating back to the first automotive assembly lines designed by Henry Ford in the early 1900s. Subsequently, work by Edwards Deming led to what is now commonly referred to as the ‘Plan/Do/Check/Adjust’ (PDCA) cycle.4 Concurrent to the development of PDCA, Juran5 developed what would become known as ‘total quality management’, which led to further developments in quality management methodology and philosophy such as Lean and Six Sigma. The same principles that apply to industry are now commonly applied to healthcare models of improvement. Unlike most research projects, QI tends to lack a true ‘control’ arm, but QI still lends itself to rigorous academic reporting. To facilitate this, the Standards for Quality Improvement Reporting Excellence guidelines were developed to provide a standard structure for reporting and publishing QI.6
Despite the growth in knowledge around QI, and the development of QI as an academic discipline, many clinicians lack the training, skills and access to resources to conduct QI. QI projects require a blend of social science, engineering and research methodology skills. Academic healthcare institutions now recognise this need, and many offer training to their medical students, residents, faculty and staff.7–9 Unlike many clinical research projects, QI projects are often smaller scale and occur on a compressed time frame.
While there are several tools to facilitate a QI project, here we focus on the standard PDCA methodology as defined by Deming. In our example, we engaged clinicians to participate by also coupling the project with the opportunity to obtain continuing medical educational credits. By aligning the QI need with the ability to meet board recertification requirements, active participation in the QI project is directly rewarded, and facilitates broader perspectives and more robust solutions.
The PDCA model follows a four-step cycle to achieve continuous improvement.10 This method is also applicable to new projects or processes, products, or services. When followed, PDCA facilitates more robust project planning, root cause analysis, data collection and review, and ability to maintain focus. ‘Plan’ signifies developing an understanding of the possible countermeasure leading to an improvement. ‘Do’ is implementing the countermeasure. ‘Check’ is analysing the data that inform the effectiveness of the countermeasure on the topic of improvement. ‘Adjust’ is applying the learning from the data analysis and either developing refinements to the original countermeasure or developing a new countermeasure.
Incorporating a tool such as ‘The Model for Improvement’ can help QI teams focus on what they are seeking to achieve. The Model for Improvement has three key questions:
What are we trying to accomplish?
How will we know if a change is an improvement?
What changes can we make that will result in improvement?
Chlamydia screening QI project for illustrating the features of a QI project
There were 1.5 million chlamydia infections reported to the Centers for Disease Control and Prevention in 2015, with nearly 80% of these being reported from outside of sexually transmitted diseases clinics.11 Adolescents and young adults between the ages of 16 and 24 account for half of these infections; they also have the highest burden of the disease in the USA, four times higher than the general public. Rates of infection have continued to increase since 2013. In 2017, the rate for women is approximately 687 per 100 000.12 The estimated annual cost of chlamydia infection in the USA is estimated to be between $250 and $770 million.13
Multiple national physician and public health groups recommend chlamydia screening for sexually active women younger than 25 years old in order to reduce the rates of infection and sequelae of the disease. These sequelae include pelvic inflammatory disease (PID), chronic pelvic pain, tubo-ovarian abscesses and infertility. There is also evidence that chlamydia infection facilitates the transmission of HIV.14 Randomised control trials have shown that screening for chlamydia can reduce PID rates.15 However, screening rates remain low.
The objective of this paper is to provide readers an overview on what resources and training programmes are recommended to support these QI endeavours. The following section provides a step-by-step process on how a specific QI project was designed and implemented to address poor chlamydia screening and treatment for young women at a large healthcare institution. Improvement in screening for chlamydia was chosen as a QI effort as this infection is the most commonly reported sexually transmitted disease in the USA, occurring at a rate of over 3265.7 cases per 100 000 in women aged 15–19, and 3985.8 cases per 100 000 in women aged 20–24.16 Untreated chlamydia infection can lead to complications such as PID, infertility and tubal pregnancy.
Methods
We used PDCA and the Model for Improvement steps to implement QI to improve chlamydia screening in women aged 16–24, and use this project as an exemplar to illustrate the steps of QI. We chose a focus on chlamydia screening due to the health burden that the infection poses, the availability of non-invasive screening tests, success of treatment and our institution’s low rates of screening which needed improvement. The chlamydia screening QI project was a multidepartment collaboration (ie, family medicine, internal medicine, paediatrics, obstetrics and gynaecology, and the University Health Service) of the University of Michigan Health System, an academic institution located in Midwestern USA. Representatives from each department worked together to produce a standard approach to develop the workflow, educational materials and a clinical decision support tool that was integrated into the electronic health record (EHR). To gain skills in QI, several members (GG and so on) of our team gained training in Lean healthcare, epidemiology and process change. For data collection we used outputs from our EHR, conducted interviews of clinicians and staff to understand the current state and challenges in chlamydia screening, and conducted clinical observations in the involved specialties. We assessed progress continually, with quarterly reporting to local clinical teams. The focus of this report is a 1-year period from 21 May 2014 to 31 May 2015.
Results
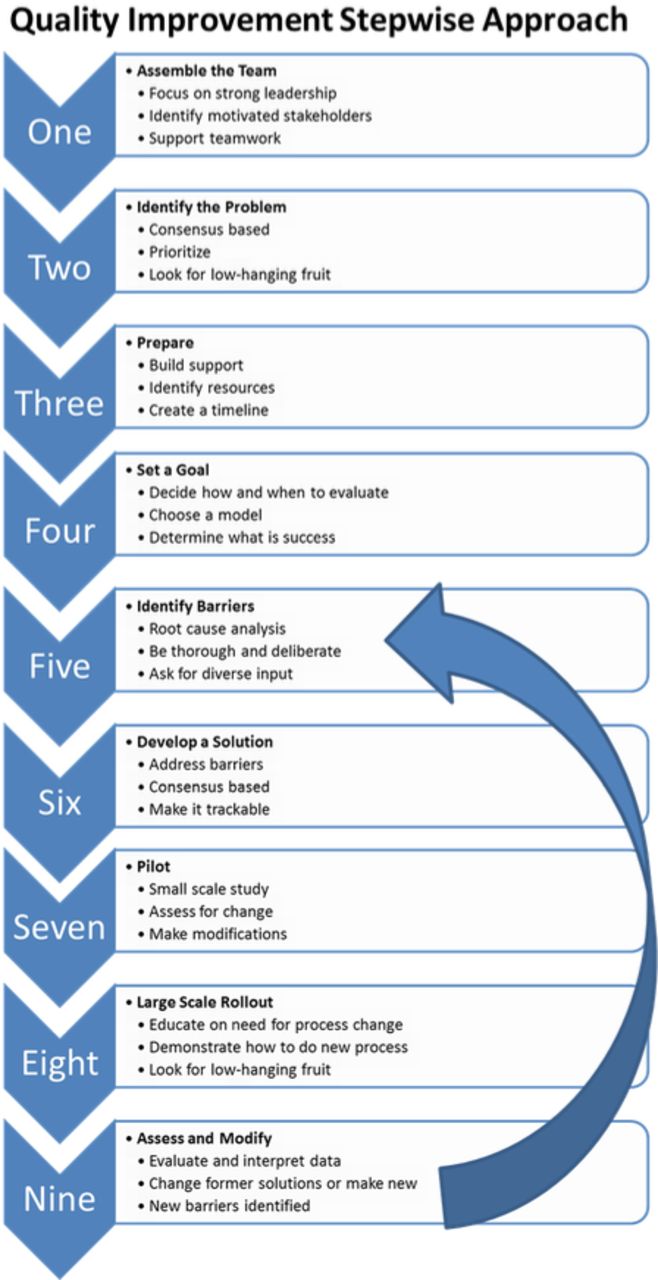
Here we illustrate nine essential steps for conducting a QI project.
Step 1. Assemble the team of stakeholders
The first step for implementing a QI project is to assemble a team of stakeholders and strong leaders (figure 1). Effective teams are diverse, interdisciplinary and share a common goal. It is critically important to have buy-in from leadership to ensure that adequate resources and time are allocated towards the proposed QI project.
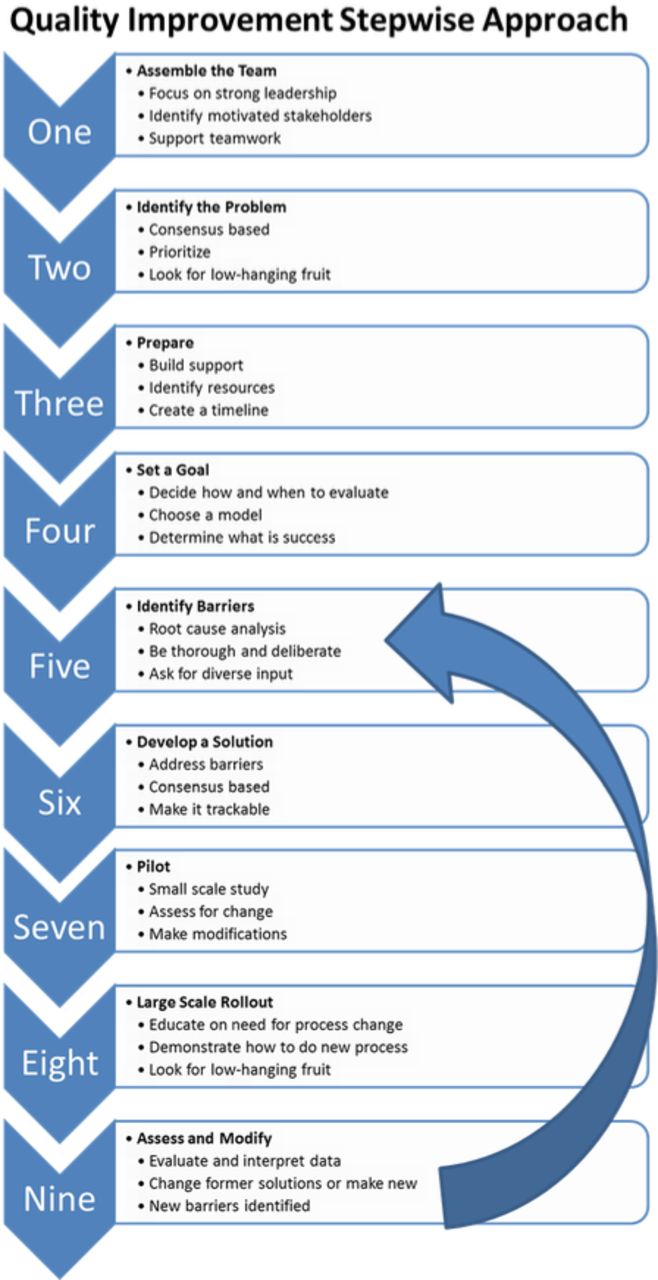
Quality improvement step-by-step chart.
In our example we engaged all primary care-based departments caring for women aged 16–24 in an outpatient setting. This allowed us to standardise screening. A team was organised by a physician leader who had Lean training as well as a master’s degree in health system administration. The team included a project manager as well as other primary care stakeholders. Selection for local project leaders focused on recruiting individuals who were respected, visible and trusted within their own departments.
Step 2. Define the problem
Through a consensus decision-making process, prioritise the highest yield countermeasures which make the largest impact with the least effort (figure 2). Methods for identifying a problem can come from chart review and clinical audit. In many places this can be facilitated through the use of EHR. Reports can be run that identify areas for improvement, for example patients needing cervical cancer screening, and these can be broken down by department, clinic and even provider. Epidemiological data can also identify problems. These could come from insurers or public health groups, for example, the Department of Public Health tracking chlamydia rates. Looking to the ‘Model for Improvement’, this step should partly answer the question of ‘What are we trying to achieve?’
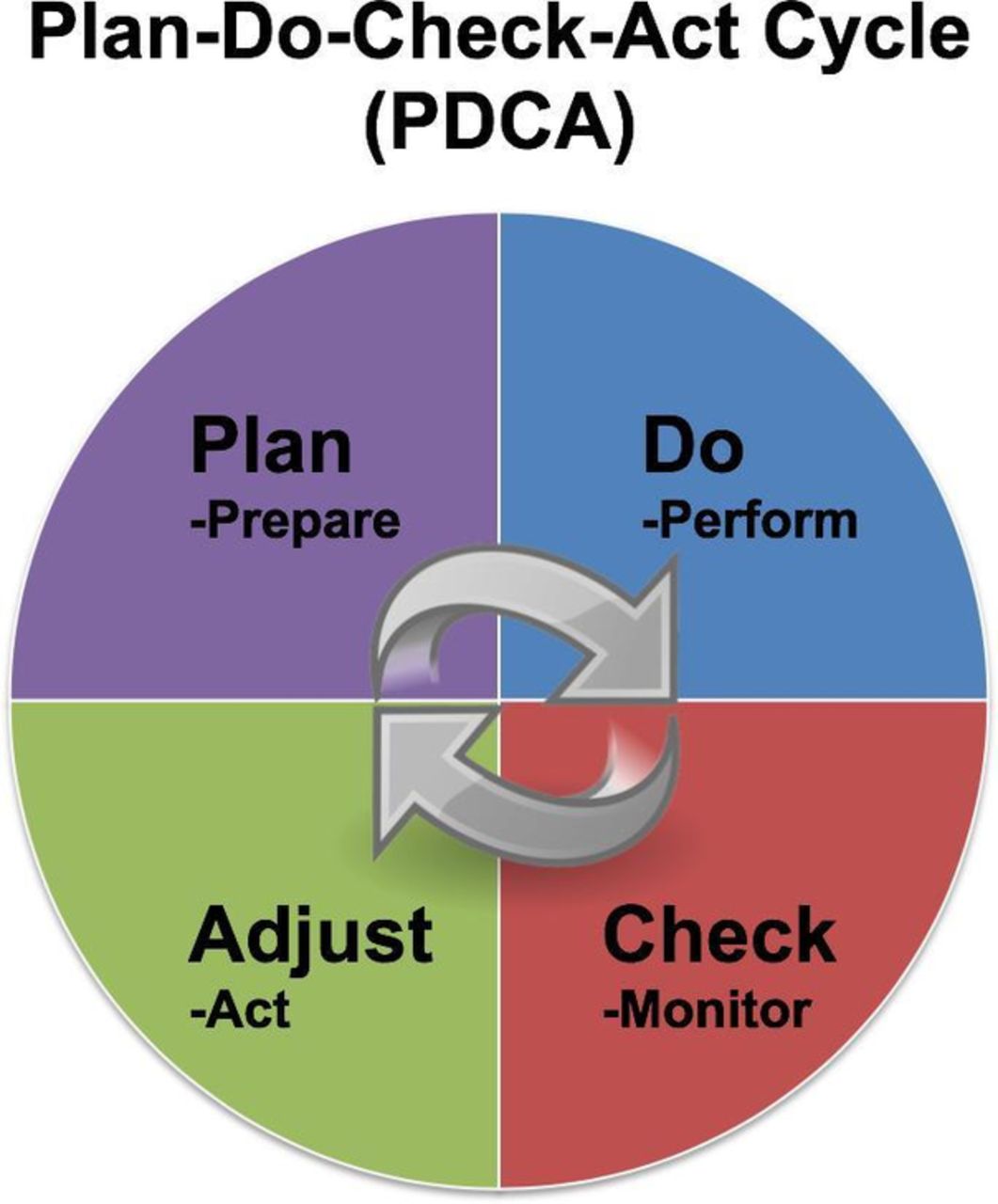
Plan-do-check-adjust graph.
When we began the project, the study practices were screening 29% of eligible patients according to the Healthcare Effectiveness Data and Information Set (HEDIS). The eligible patients were women aged 16–24 who were deemed sexually active by a HEDIS algorithm. Our problem was defined as underperforming on chlamydia screening for women aged 16–24 years old.
Step 3. Identify stakeholders to build support for the project and assess level of interest
The next step is to prepare for the project (figure 2). Research examples of similar projects and look for resources such as clinical guidelines to assist in developing your solution. The team needs to decide on a budget and timeline, determine if relevant data are already being collected, and establish what are the baseline data.
Our team began by identifying and recruiting clinician leaders from each of the stakeholder departments. From here we coordinated the work both with the operational leadership and clinical leadership of the local clinics as they would be responsible for insuring the process was in place and functioning. We also paired this QI project with the Part IV Maintenance of Certification (MOC) credit through the American Board of Medical Specialties Multi-Specialty Portfolio Program (MSPP).17 An MOC project through MSPP provides physicians required credit towards maintaining board certification by conducting a QI project using the PDCA methodology. Additionally, we identified a toolkit for improving chlamydia screening.18 The Agency for Healthcare Research and Quality has several examples on their website.19
Step 4. Determine a goal and decide how to assess progress towards the goal and achievement of success
This involves deciding on a goal that is concrete, measurable, achievable and clinically important. This should be a discussion among the stakeholders, as what is important or achievable for one group may be different for another. Decide how to measure progress towards the goal, for example having monthly reports on screening rates that are reviewed by the stakeholders. This step fits into the ‘Model for Improvement’ under the first two questions noted in the Introduction section.
Our goal was to screen 57% (HEDIS 95th percentile) of eligible patients. Our measure of interest was the proportion of female patients aged 16–24 who had a chlamydia screen in the last 12 months. We planned to evaluate the project during an initial pilot period and once it was rolled out to all clinics, using the PDCA methodology. We agreed to meet monthly to review department-level data to allow for any further adjustments as needed. One example of an adjustment was changing the workflow to have a urine sample collected for any eligible patient prior to the visit. A model such as the above helped the team stay focused even in chaotic and demanding healthcare environments in which schedules and resources changed from day to day.
Step 5. Identify barriers
This can be done through brainstorming with stakeholders, surveying staff and through a root cause analysis (figure 2). Physicians and non-physicians tend to jump to solutions instead of doing a root cause analysis. Root cause analysis is important to do so that the solution is sustainable. Root causes are underlying, can be controlled and managed.20 They explain the what, why and how something occurs. The analysis involves data collection, recommendations and implementation very similar to the PDCA cycle. This process is slow and must be deliberate in order to create a new normal and ensure sustainability. This step addresses the ‘Model for Improvement’s’ last question.
In our case simply telling physicians to increase chlamydia screening will not work. The entire process must be changed. Some of the barriers we were able to identify were lack of knowledge of the screening recommendation, lack of knowledge of a non-invasive urine test for screening (no requirement for a pelvic exam), fear of breaking confidentiality for minors, not understanding the process of insurance coverage and insurances’ explanation of benefits to the parents of minors, discomfort discussing sexually transmitted infections during a clinic visit, lack of time in the visit to address sensitive issues, and a lack of a standardised approach to screening.
Step 6. Develop a countermeasure
As with defining the problem, a consensus among the team is crucial for success of the solution. This step is made easier when the problem and barriers have been clearly defined. The potential solution(s) must address the underlying causes of the problem. Solutions will also be more robust with input from the whole team. For example, if the front desk staff is responsible for giving patients information on screening, then input on how this is done best comes from them. There likely will be multiple solutions and they may vary by stakeholder.
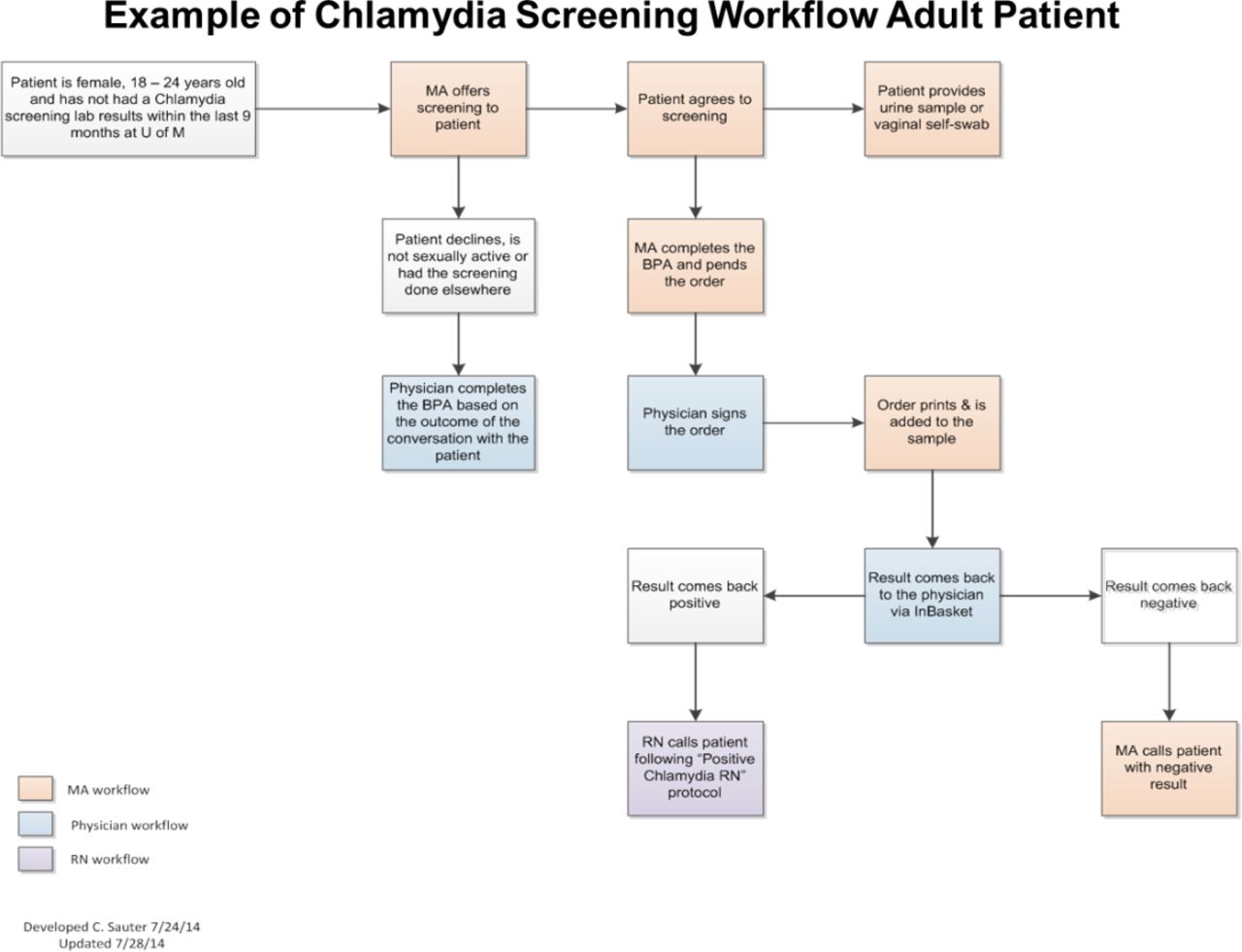
We developed a standard approach for workflow, educational materials and a clinical decision support tool within the EHR to overcome our obstacles to screening. While not required for all QIs, a workflow was essential to our project.21 The workflow streamlines discussion of screening, collection of screening sample, ordering test, follow-up of results and treatment. Because the workflow is standardised and easily visualised in the included flow sheet, it can be readily adapted to other clinical sites. The newly developed educational materials for staff, patients and parents explained the importance of screening, as well as the process for screening, and notification of results and treatment. These materials are also easily transferable to other sites. Lastly, the clinical decision support tool was an alert that is displayed in an area of the EHR called ‘best practice advisories’ (BPA). This notification is visible whenever the chart of an eligible patient is accessed. The automated alerts can easily be transferred to any healthcare system using an Epic EHR system (figure 3).
{kind=link}
{kind=link}
{kind=link}
Example of Chlamydia screening workflow. BPA, best practice advisories; MA, medical assistant; RN, registered nurseof M, University of Michigan.
Step 7. Test the process in a limited setting
Assessing the results and modifying the process on a small scale helps inform how the project is working (figure 2). Typically, this involves conducting a pilot project. This is like a mini-PDCA cycle within the larger PDCA cycle of your QI project. This is where to test your initial problem, barriers, solutions and data collection, identify new barriers and solutions, and refine your process.
We carried out a pilot in three of our clinics: one family medicine, one paediatric and one internal medicine. These departments had representatives on the chlamydia QI team which facilitated the introduction and monitoring of the project. After 8 months the pilot clinics improved their chlamydia screening to 60% of eligible patients. During this time, feedback from the three clinics was used to adjust the process. For example, in paediatrics they felt that the discussion around chlamydia testing was too burdensome for all office visits given their high percentage of minor patients. They elected to use the workflow for chlamydia screening, and have the EHR alert, only during well-child exams rather than at all visits.
Step 8. Large scale project rollout
As illustrated in figure 1, evaluating and modifying the project is a critical process more than a single step (figure 2). This involves review of the data by the project team and by those who are doing the work, that is, medical assistants, office managers, physicians and nurses. All participants should be encouraged to provide feedback on the process, new barriers and new solutions. This can be done by surveying or interviewing the staff and by reviewing internal policies.22–24
Following modifications informed by our pilot, we launched the project by activating the BPA and providing educational materials in all primary care clinics. This included presentations to educate the clinical providers and staff on the importance and need for process change to improve our low chlamydia screening rates. These occurred in the participating departments in large and small settings, for example at Grand Rounds as well as at medical assistant meetings for individual clinics.
Step 9. Evaluate and modify the QI project
As illustrated in figure 1, evaluating and modifying the project is a critical process more than a single step (figure 2). This involves review of the data by the project team and by those who are doing the work, that is, medical assistants, office managers, physicians and nurses. All participants should be encouraged to provide feedback on the process, new barriers and new solutions. This can be done by surveying or interviewing the staff and by reviewing internal policies.22–24
We met monthly to discuss the results from each of the participating departments. Shortly after a standard workflow and BPA had been implemented, the screening rate for women between 16 and 24 years old improved to 66% of eligible patients in family medicine clinics. We noticed an immediate improvement as soon as the process went live, and hypothesised the build-up and discussion of the project led to improvement before the process actually changed.
Additional barriers across departments identified were lack of adoption of the standard workflow among check-in staff, medical assistants and physicians. Our intervention to address this barrier was to standardise medical assistant workflow from intake to utilisation of the BPA particularly when the patient is 16–17 years old. A new standard workflow was agreed on and disseminated to each clinic. Two months after this intervention, our screening rates for 16–17 years old improved from 42% to 48%. Significantly, 4 years after our intervention, we have been able to maintain the rates of chlamydia screening well above our initial rate of 29%.
Discussion
QI projects benefit from the step-by-step process outlined in the PDCA and Model for Improvement theories to effectively tackle potential challenges and improve the overall project’s relevance and success. The scale of the QI project can vary from a single clinical site to a large multispecialty group as the above example used. For example, Wakai et al 25 conducted a QI project in a single site but included an intervention. Focused on improvement of periodic assessments, they identified and addressed barriers and threats to the project’s success. QI projects can benefit from a mixed-methods approach, combining quantitative and qualitative analyses to better determine the next steps to the QI process.22
Regardless of the model or the design used by the QI project, effective communication with all involved parties is key to successful QI projects. In hindsight, our project might have been more effective if we had communicated with our Department of Public Health about our change in approach to chlamydia screening. For example, in 2015, chlamydia incidence reached a record high prompting the Department of Public Health to declare an epidemic. The rate of positive screening tests was tracked by our microbiology lab and remained between 3.3% and 3.6%, although the number of tests increased by nearly 10 000 in 2015 compared with 2014, the year of our intervention. The increased positive tests were likely related to our increased screening efforts rather than a true outbreak.
Four years after intervening, the rates for chlamydia screening in our clinics ranged between 49% and 80% for 18–24 years old but 32%–63% for 16–17 years old. This is remarkable as achieving screening rates above 55% is difficult even in a research setting.26 Despite the success in increasing screening rates for chlamydia, certain groups (ie, younger aged females) were still low. This highlights that QI projects may necessitate additional QI projects to address areas of concern that were discovered. For example, it was quickly noted that screening rates for 16–17 years old remained lower than for 18–24 years old. These data were not initially separated prior to our QI project or at the start of our intervention, limiting the ability to fully address this issue. We did however identify unique barriers mainly with the paediatric department that required modifications from the standard workflow that was working effectively for the chlamydia screening programme in other departments. The younger women, aged 16–17 years old, have special considerations for confidentiality, privacy and explanation of benefits forms designed to prevent accidental parent disclosures. In light of these findings, we plan to complete another MSPP MOC project for chlamydia screening to fully address these issues.
QI projects, including the one described above, have the ability to change healthcare delivery systems. Our QI project demonstrated the importance of chlamydia screening to the clinicians, and provided a feasible way to deliver care effectively to women aged 16–24 when coming for medical appointments. The use of a well-integrated BPA decreased clinicians’ mental demands by simply reminding and offering them of an evidence-based screening recommendation that could be selected with a single click.
There are several challenges and limitations to conducting QI projects. These projects require special skills that many clinicians lack. Furthermore, QI projects, similar to other research projects, need time, resources and commitment from multiple involved parties to successfully complete. The development and the design of QI projects should be carefully thought out, including how the project will be implemented, assessed, if needed, modified and communicated to others. QI projects, if not carefully designed, can be doomed by insufficient training or participation of all involved parties, poor fit with existing structural clinical flow or a perceived low priority of the project (eg, not a relevant or significant clinical issue). Also, if publication is a possibility, institutional review board approval should be requested.
Other resources
The Society of Teachers of Family Medicine (STFM) Conference of Practice Improvement is provided annually and features practical skills and resources for practice change. The STFM also has a rich online resource catalogue of courses, presentations and handouts on QI. Some academic institutions cover courses in business, public health and/or engineering schools. Furthermore, international organisations such as the World Organisation of National Colleges, Academies and Academic Associations of General Practitioners/Family Physicians27 are committed to the improvement of patients’ quality of life and have offered QI workshops in the past.28
Conclusions
Incorporating QI training programmes is a good investment for healthcare organisations and academic centres since they generate useful projects that will likely positively impact the overall healthcare system and improve dissemination of helpful and high-quality clinical strategies. The QI approach presented here can be applied to a myriad of clinical scenarios. Potential areas for improvement include any disease with a screening recommendation, for example lung cancer screening with low-dose CT scan. This project could also work for situations other than screening, such as triage of patient phone calls to clinic, or increasing uptake of the human papillomavirus vaccine. While QI projects require commitment and resources, as demonstrated here, these projects have the potential for primary care physicians to improve the health of the entire populations.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was deemed not regulated by the University of Michigan Institutional Review Board.
Provenance and peer review Not commissioned; internally peer reviewed.