Article Text

Abstract
Objective Social prescribing is a person-centred model of care with emphases on lessening the impact of unmet social needs, supporting the delivery of personalised care, and reducing non-medical resource use in the primary care setting. The purpose of this systematic review was to synthesise the effect of social prescribing for older adults within primary care.
Design We followed standard systematic review guidelines, including protocol registration, screening studies (title/abstract and full text) and assessing the study quality.
Eligibility and information sources We searched multiple online databases for studies that included older adults 60+ years (group mean age), an intervention defined and called social prescribing (or social prescription) via health provider referrals to non-medical services, and quantitative physical and psychosocial outcomes and/or health resource use. We included experimental and observational studies from all years and languages and conducted a narrative synthesis. The date of the last search was 24 March 2022.
Results We screened 406 citations (after removing duplicates) and included seven studies. All studies except one were before–after design without a control group, and all except one study was conducted in the UK. Studies included 12–159 participants (baseline), there were more women than men, the group mean (SD) age was 76.1 (4.0) years and data collection (baseline to final) occurred on average 19.4 (14.0) weeks apart. Social prescribing referrals came from health and social providers. Studies had considerable risk of bias, programme implementation details were missing, and for studies that reported data (n=6) on average only 66% of participants completed studies (per-protocol). There were some positive effects of social prescribing on physical and psychosocial outcomes (eg, social participation, well-being). Findings varied for health resource use. These results may change with new evidence.
Conclusions There were few peer-reviewed studies available for social prescribing and older adults. Next steps for social prescribing should include co-creating initiatives with providers, older people and communities to identify meaningful outcomes, and feasible and robust methods for uptake of the prescription and community programmes. This should be considered in advance or in parallel with determining its effectiveness for meaningful outcomes at multiple levels (person, provider and programme).
- Aging
- Primary Health Care
- Social Determinants of Health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Social prescribing is a complex health and social model of care. Older adults may particularly benefit from this model of care.
WHAT THIS STUDY ADDS
We identified only seven published studies specifically for older adults, implementation data were frequently missing and there were some challenges for participants’ uptake and adherence to programmes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This synthesis provides a discussion for providers, researchers and policy makers to consider when developing future practice-based research studies for older adults and social prescribing.
Introduction
The impact of environmental and social factors on health is not a new phenomenon but is even more relevant today. Decades ago, population-level research such as the Whitehall Studies of British Civil Servants1 highlighted the importance of the social determinants of health, defined as ‘the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life’.2 The WHO’s 1986 Ottawa Charter for Health Promotion3 identified health-promoting strategies such as supportive environments and strengthening community action.3 Addressing social needs is especially important now because of the COVID-19 pandemic putting people at risk for social isolation.4 Social prescribing is a model of health and social care that aims to mitigate some of the effects of unmet social needs. Although early concepts of social prescribing were situated in low resource communities for people impacted by physical and psychosocial concerns, more recent studies have included people living with long-term health conditions and/or loneliness, for example.5
What is social prescribing? It is a complex health and social model of care that aims to use a person-centred approach to connect people with unmet non-medical needs to community assets (public or private). Community assets are the available resources in the physical environment, and people and social connections. Other names for social prescribing include social prescription, community referrals or non-medical prescribing. In the UK publicly funded system, there were elements of social prescribing initiatives since the 1980s, but it was only recently funded as part of the 2019 National Health Service (NHS) Long Term Plan.6 Other research highlights smaller scale social prescribing initiatives outside of the UK, such as in Australia7 and Canada.8 In a recent discourse analysis, Calderón-Larrañaga and colleagues9 summarised three main conceptualisations with potential limitations for social prescribing. These include to: (1) reduce the burden of unmet social needs by shifting non-medical care to the social and community sector; (2) reduce the heavy workload experienced by primary care providers (PCPs) by empowering people’s self-management skills; and (3) support delivery of personalised care in primary care. They propose social prescribing ‘as a solution’ should refocus from impacting the healthcare system to ‘evaluating the extent to which SP may (or may not) succeed to support people in greatest need while contributing to stronger, fairer healthcare systems’ (p.863).9
What does social prescribing look like in practice? Although there is no one accepted definition (or operationalisation) for social prescribing, there are at least four primary care pathways with varying levels of support and interactions.10 For example, the PCP who: (1) provides information on a community programme (signposting); (2) makes a direct referral for the person to a community programme; (3) connects the person to a navigator (community link worker); and (4) connects the person to a community link worker within a centralised hub of people and resources.10 Social prescribing is similar to other personalised care programmes such as reablement11 or green/physical activity PCP prescription innovations.12 13 The unique features of some social prescribing pathways include the: (1) inclusion of a community link worker to support people in the identification, uptake and long-term engagement with community programmes and resources; and (2) the focus on activities beyond exercise and/or physical activity.
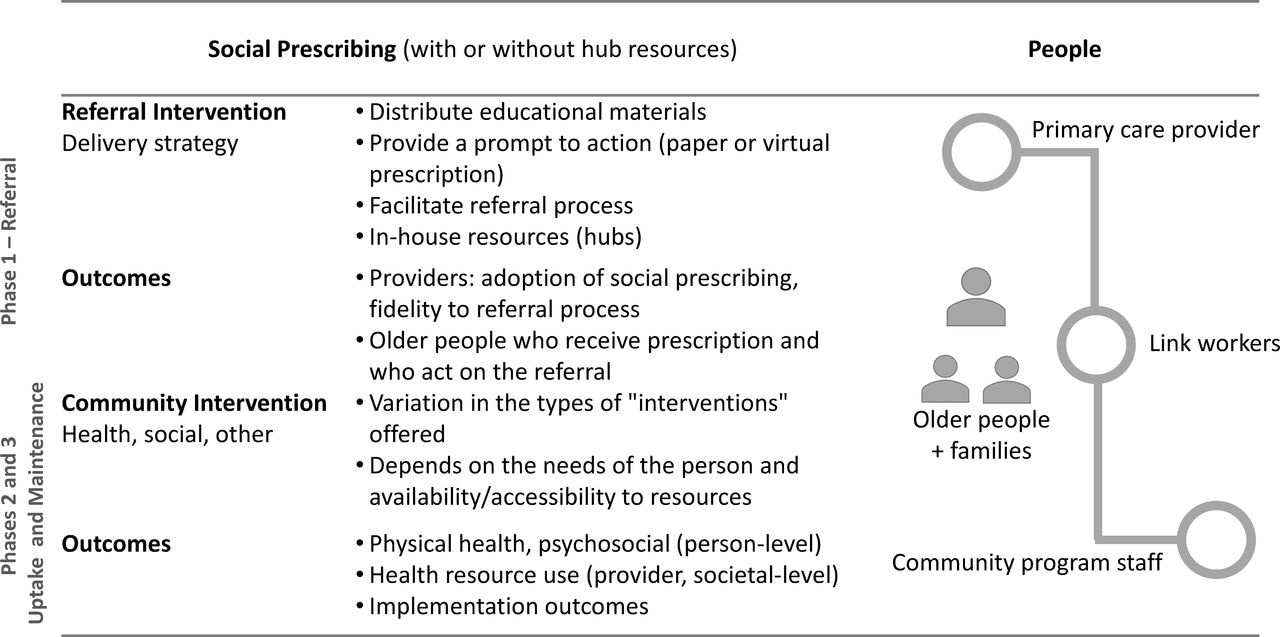
Deconstructing social prescribing. Social prescribing has elements of complexity across several domains: interventions, implementation, context and populations.14 Husk and colleagues10 reported on three (behaviour-related) phases of social prescribing: enrolment, engagement and adherence. Specifically, it consists of a referral ‘intervention’ to support people (eg, awareness and uptake) to receive community-based ‘interventions’ (eg, programmes such as social groups, physical activity etc, or services such as access to food and housing) based on identified needs. Outcomes (at person/provider/systems level) can be affected if the referral was adopted (or not) and delivered as intended (fidelity) by providers. At the person level, some factors to consider are acceptance and uptake of the referral by the person and/or if they do or do not maintain behaviours. There are similar implementation factors to consider for link workers and the people running/providing the community programmes or resources (please see figure 1). However, despite the complexity of social prescribing, few studies discuss it from this behavioural15 and/or implementation science perspective.16
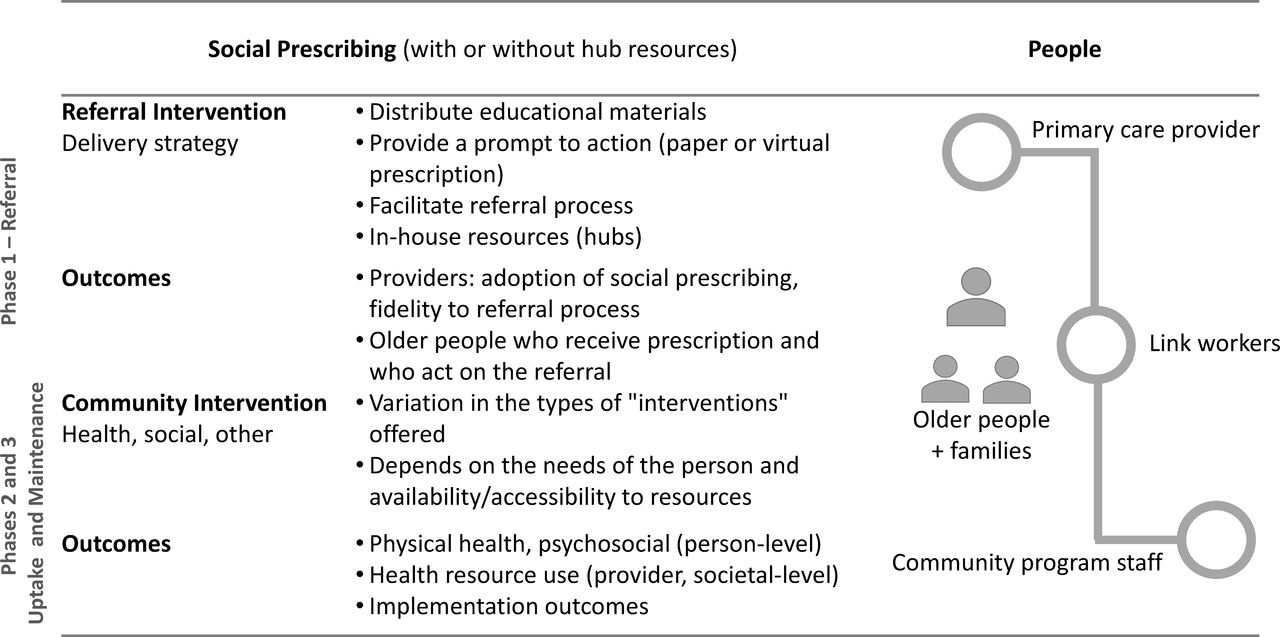
This figure outlines people involved and three main components for social prescribing: (1) the referral process; (2) the engagement or uptake phase when the person attends the community programme via working with a link worker; and (3) maintenance of the new behaviour or activity. Finally, the figure describes types of possible outcomes (implementation vs health/social/health resource use).
How might social prescribing ‘work’? Recent work has aligned social prescribing with the social identity approach (from social psychology), which discusses the effects of relationships on health and well-being.17 Calderón- Larrañaga and colleagues in their realist review propose mechanisms for social prescribing (ranging from individual to policy levels), many of which are behavioural (eg, buy-in, informed interaction, support, leadership) and organisational (eg, accessibility, culture, stable funding). They further describe social prescribing ‘best practice’ by the people involved. For example, they discuss social prescribing is best delivered when the PCP takes an integrated approach, the link worker develops relationships (and not a set number of visits) and the community resources were available and flexible.18 Social prescribing is still evolving, with foundations in person-centred and relationship-centred care, and social and behavioural psychology,19 but there is a need to elucidate how social prescribing may ‘work’ in practice.
Social prescribing and older adults. Older adults are at high risk for experiencing the negative physical and psychosocial impacts of social isolation and loneliness,20 and therefore, this population may particularly benefit from social prescribing programmes. For older people, social isolation and loneliness are linked to deleterious physical and psychosocial outcomes21 leading to possible life challenges for people and their families. Older adults experiencing social isolation or loneliness (even moderate amounts) may be at higher risk of developing frailty.22 Furthermore, people who are socially isolated are more frequent users of medical services.23 Although older adults encompass a large and diverse age group, they may have unique preferences or challenges for social prescribing (compared with younger populations) to support connection back to the community. There are systematic reviews on social prescribing,15 16 24–32 but only one review29 by Smith and colleagues29 was specific to older adults with frailty. However, the authors did not locate any eligible studies and concluded there was a paucity of evidence evaluating the effectiveness of social prescribing programmes for older adults with frailty.29 Studies on social prescribing are increasing, and therefore, it is timely to review evidence for older adults.
Thus, in this systematic review of peer-reviewed studies, our primary aim was to synthesise available quantitative evidence on the effectiveness (efficacy) of social prescribing with older adults (group mean age 60 years and older) within a primary care setting. A secondary aim, where possible, was to synthesise how the interventions were implemented (eg, the referral process and community programmes) and if participants used the social prescription (participation after referral) and maintained new behaviours (programme adherence and completion).
Methods
This was a systematic review guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).33 We registered the protocol with PROSPERO prior to starting the review, and it is available at PROSPERO 2021 CRD 42021290233 . Our primary research question was: in primary care, what is the effectiveness of social prescribing on physical and psychosocial outcomes and health resource use of older adults? We initially wanted to explore the similarities and differences of studies conducted before and during the COVID-19 pandemic to describe if and how social prescribing changed, but there were not enough data to answer this question.
Search strategy
We reviewed several previously published systematic reviews on social prescribing to understand the scope of the evidence base.15 16 24–32 We then searched the following electronic databases: EBSCO (Cumulative Index for Nursing and Allied Health (CINAHL) Complete; APA PsycArticles and PsycINFO; and SPORTDiscus); Cochrane Controlled Trials and Cochrane Database of Systematic Reviews; Embase; MEDLINE Ovid; and Google Scholar (advanced feature title only). Please see table 1 for database search strategies. We also conducted a forward citation and backward (reference list) search for included publications using Web of Science and Google Scholar. We conducted our initial search on 1 December 2021 and the last search on 24 March 2022.
Systematic review search strategies for selected databases
Eligibility criteria: we used the following concepts defined by our research question: population (studies with the group mean age 60+ years); intervention (social prescribing); comparator (any or no intervention); and outcomes (physical and psychosocial outcomes and health resource use). We only included studies if the authors called the intervention social prescribing or prescription. We included experimental studies (randomised controlled trials) and observational studies (cohort, case–control, cross-sectional) from across all years and languages. We excluded reviews, editorial, commentaries, letters, theses and protocols. Other exclusion criteria were non-peer-reviewed publications, and studies that did not call their intervention or programme ‘social prescribing’ or ‘social prescription’.
Selection process
After running the search strategy, author AP uploaded citations to Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia). Authors AP and MCA independently screened all citations retrieved from searches at level 1 (title and abstract) for inclusion in the study. Following this step, the same two authors reviewed full-text publications (level 2) to determine the final list included in the systematic review. The plan was to consult another author if there were any unresolved discrepancies in adjudication.
Data collection process
AP and MCA developed the data extraction sheet in Excel through an iterative email process. AP extracted data and MCA checked 10% for accuracy. A priori, we decided if errors were noted; a second author would check all extracted data. A final data check was completed prior to submitting the manuscript for peer review.
We extracted the following information: first author, year, location, study design, time points, sample size, group mean age, education, ethnicity, gender, socioeconomic status (person and/or community), community asset referral process, social prescription, duration of intervention, outcomes, findings, programme implementation factors, adverse events, missing data, and funding and conflict of interest reported. We referred to PROGRESS-Plus to guide data extraction for participants’ characteristics.34 35 We used NVivo (QSR International Pty Ltd, Melbourne, Australia) to search the abstract and discussion sections to code authors’ statements on study limitations and suggestions for future research. To understand if/how our synthesis compared with other reviews, we conducted a forward citation search using Web of Science or Google Scholar to determine if the included primary study was cited in other published systematic reviews.
Outcomes of interest
We included studies with any related quantitative measures of physical or psychosocial outcomes including well-being (individual level) and health resource use (system level). We also extracted data on how social prescribing was implemented (eg, who made referrals, presence of link worker, uptake of referral, etc).
Quality assessment
We initially proposed to use the Cochrane Risk of Bias Tool36 for randomised controlled trials and the ROBINS-I Tool37 for non-randomised studies. Based on the type of study designs identified for this review, these tools were not ideal; therefore, we used the National Institutes of Health (NIH) Quality Assessment Tool for Before–After (Pre–Post) Studies With No Control Group,38 even though one study had a control/comparison group (data from people who declined to participate in social prescribing). The tool consists of 12 questions, and the possible responses are: yes, no, cannot determine, not applicable or not reported. The tool’s aim is to assist the reviewers to evaluate a study’s internal validity and risk for bias. It does not provide a final score based on the sum of responses for each question.38 However, an overall rating is determined as good, fair or poor. AP and MCA independently reviewed each study using the assessment tool questions, then met to determine final ratings.
Synthesis methods
Based on the identified evidence, we conducted a qualitative (narrative) synthesis using the Cochrane’s Synthesis Without Meta-analysis (SWiM) guidelines.39 We first reviewed the nine SWiM steps and confirmed: the process of grouping studies; the synthesis method (eg, summarise effect sizes and/or voting counting direction of effect); we would not exclude studies based on quality assessment; data visualisation; and what and how to report findings. We used NVivo to identify and code information within included studies.
Review team composition and experience
Team members have experience in health and social care models and synthesis methodologies. We consulted a university librarian to confirm choice of quality assessment tool. No authors of this systematic review participated in any of the included studies.
Results
Study selection
We conducted the search at the end of 2021 and completed the final primary search on 12 January 2022. We conducted the forward and back citation searches on 24 March 2022. We identified 574 citations, of which 168 were duplicates. We screened 406 citations at level 1 and 69 publications at level 2. Seven studies were included in the synthesis40–46; all studies except one46 were published in 2017 or later. Figure 2 is an overview of the screening process summarised in the PRISMA flow diagram.

PRISMA 2020 flow diagram.33 PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
Table 2 and figure 3 provide a summary of the seven included studies.40–46 All studies except one44 were before–after studies without a comparison (control) group, and all except one study43 was conducted in the UK. Data collection (baseline – final) occurred on average 19.4 (14.0) weeks apart. Some studies were based on data collected within an existing community programme of social prescribing.40 42 44 Other studies were more focused on a specific population or type of community programme, for example, a social programme for older people with dementia and their family caregivers41; for older people living in rural communities during the pandemic43; a museum-based programme for older adults45; and an arts-based programme for older people with sensory impairments.46 Two studies reported costs for attending programmes.41 42

Summary outlining features of included studies based on target population, health provider referral source, community assets and outcomes evaluated in the studies. Please note some studies included more than one option for social prescribing community assets.
Studies had a mean (SD) 74.4 (55.1) number of participants (range 12–159) at baseline. Most studies included more women than men: percentage of women in studies ranged from 36% to 100%. For studies that reported mean age (n=5), the mean (SD) age was 76.1 (4.0) years. Three studies included family caregivers.41 42 46 Only the study by Thomson and colleagues45 reported on ethnicity: ‘82% white British’, n=115, and no studies reported on participants’ level of education. Three studies did not report socioeconomic factors.43 44 46 For the study by Thomson and colleagues, an exclusion criteria was participants could not be in any paid or voluntary employment (full time or part time).45 In the studies by Elston and colleagues40 and Jones and colleagues,42 researchers did not directly study socioeconomic status, but the social prescribing programmes were set in areas with some level of deprivation and/or the programme aim was to address inequities, especially for people living on low income. Only the study by Giebel and colleagues41 included people living on low income: most participants lived in quintile 1 and 2 (most deprived) neighbourhoods as measured by the UK-based Index of Multiple Deprivation score.
Outcome measures reported were categorised into three main areas: physical (two studies40 42), psychosocial outcomes (six studies40–43 45 46) and health resource use (three studies40 42 44) (table 2, figure 3).
Description of included studies using the PICO framework
Citations in other systematic reviews
Based on a forward citation search, we identified all except two studies42 43 were included in other systematic reviews with participants across age groups: Elston,40,15 24 Giebel,41,15 Loftus44,15 28 31 45 and Vogelpoel.46,24 28 31 The study Elston (2019) was mentioned in the only systematic review of older adults and social prescribing,29 but it was excluded from the analysis because it did not specifically recruit people who were frail or prefrail. Since the 2019 systematic review,29 at least three studies were published.41–43
Quality assessment
All included studies except one by Loftus and colleagues44 used a before–after research design without a control group and therefore were at risk for bias. Loftus and colleagues44 compared participants’ results with those from people who declined social prescribing (within the same study). Based on the NIH Quality Assessment tool (possible rating of good, fair or poor), three studies were rated as good,40 42 44 three studies were rated as fair41 43 45 and one study was rated as poor46 (table 3).
Reported psychosocial results from included studies⇓
Program implementation factors
We extracted data (when available) on factors related to delivery, uptake, dose and adherence to the social prescribing programmes.
Referral source and community assets: studies consistently reported the referral source from health and social providers; physicians were mentioned in five studies.40 41 43 44 46 Community assets prescribed included arts and museum programmes, physical activity, social-based activities and combined programmes (table 2, figure 3).
Uptake of referral: only the study by Loftus and colleagues44 reported on the number of people who participated in a programme after the referral. Specifically, 68 people were referred, but only 28 people (41%) participated in a social prescribing activity.44 Reasons for declining the referral were change of mind, deterioration in health, no activity available and other reasons.44
Adherence to community programme/research: six studies reported on completion of the programme and/or research.40–44 46 For all studies reporting adherence to programme/final assessment, the range of percentage of participants who completed studies was 41%–68%. However, including the study by Loftus and colleagues44 with a per-protocol perspective, the range of percentage of participants who completed studies was 42%–100%; on average, only 66% of participants completed studies (per-protocol).
Dose/volume of activities: in the study by Giebel and colleagues,41 participants made between 1 and 36 visits; in the study by Jones and colleagues,42 participants attended, on average, 19 sessions over 16 weeks; and in the study by Kim and colleagues,43 10 participants completed all 10 programme sessions.
Other factors: only the studies by Elston and colleagues40 and Jones and colleagues42 discussed participants’ goals. Only one study, by Jones and colleagues, stated ‘no unintended outcomes’42; otherwise, there were no reports of assessing for harms related to the interventions.
Results of syntheses
Physical outcomes (two studies): both studies with physical outcomes had a ‘good’ quality rating.40 42 In the study by Elston and colleagues,40 participants significantly increased their activity and the frailty measure decreased. In the study by Jones and colleagues,42 32/66 (48%) participants self-reported ‘frequent physical activity’.
Psychosocial Outcomes (six studies): study quality of the studies was ‘poor’ to ‘good’. Two of nine reported psychosocial results were statistically different at follow-up. Jones and colleagues42 provided the number of participants who self-reported an increase in social connection (14/66, 21%), improvement in health status (13/66, 20%) and higher confidence (15/66, 23%).
Health resource use (three studies): all three studies reporting health resource use were rated as ‘good’ quality. There was an increase in healthcare costs following the intervention in the study by Elston and colleagues,40 and in the study by Loftus and colleagues,44 there was a significant decrease in general practitioner (GP) visits in the intention to treat analysis (n=68), which was no longer significant in the per-protocol analysis (n=28). In the third study reporting health resource use by Jones and colleagues,42 there was a reduction in the number of GP attendances by 19 appointments. This study also reported social prescribing resulted in social return on investment of £5.07 of social value generated for every £1 invested.42
Tables 3 and 4 are findings reported for psychosocial outcomes and health resource use, respectively.
Reported health resource use results from included studies
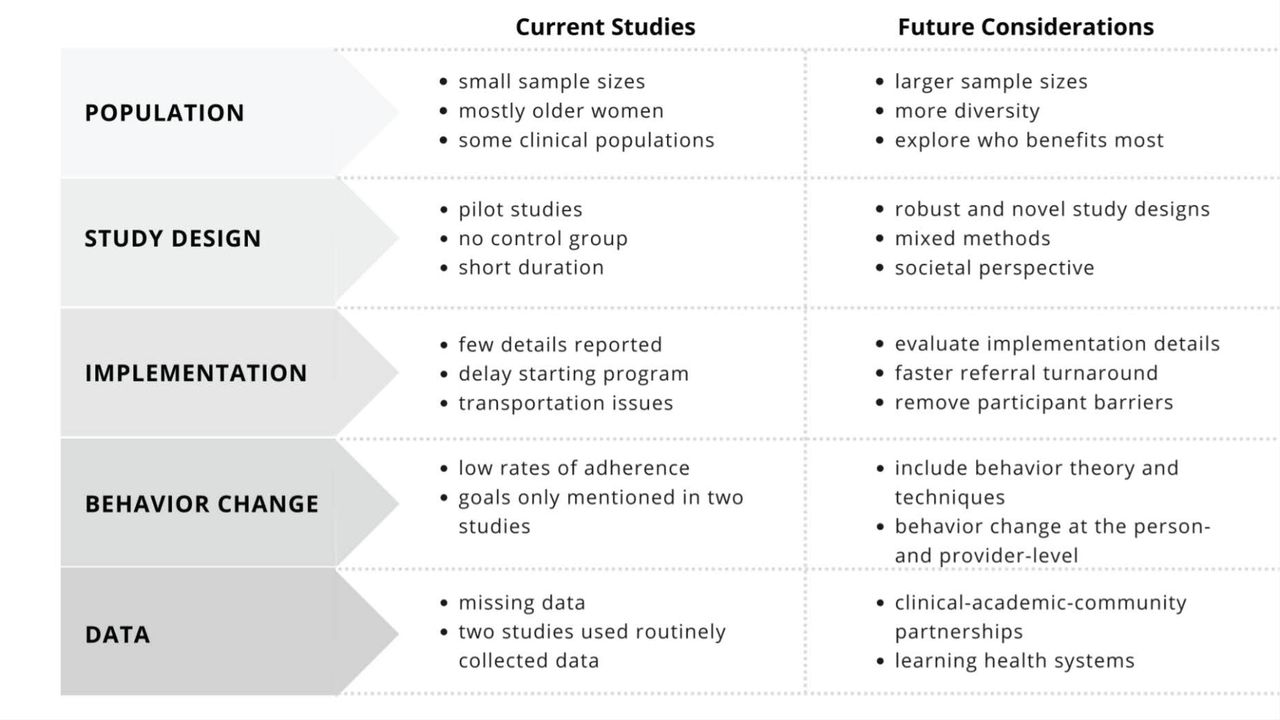
Figure 4 is a summary of key points extracted from the abstract and discussion sections of included publications, alongside our additional points based on the synthesis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of (1) included studies of older adults and social prescribing limitations and (2) future considerations. Points were based on information located within publications with additional points suggested from overall results.
Discussion
Social prescribing aims for person-centred care embedded within a community setting and is an increasingly important model of care given the past few years of living with the inequities and social consequences of the COVID-19 pandemic. This systematic review provides a novel perspective by focusing on older people and social prescribing, as they may have different capacities, opportunities and motivation to engage in community-based activities and programmes. Furthermore, barriers may be more salient for some older people, such as deterioration in health status44 including mobility46 and lack of transportation.41 Nonetheless, older adults are a large and diverse group; thus, it is not a ‘one size fits all’ approach to social prescribing referrals or community assets. Yet, in our review, we note few peer-reviewed studies of social prescribing for older adults. Available studies were small, almost all included before–after designs without a control group, had missing data and low rates of adherence, and implementation factors were not routinely provided within publications. However, this synthesis provides clues for moving forward and presents an opportunity to create a road map for a practice and research agenda for social prescribing with a focus on older adults.
Evidence from this synthesis includes a few positive physical and psychosocial outcomes (participation and well-being) for older adults and social prescribing, but the findings varied for health resource use. As social prescribing is an emerging model of care, these results highlight feasibility and contribute to the development of next steps. The findings of increased reports of participation and well-being (even in a before–after study design) suggests the referral model and community asset programmes may hold some appeal, although this remains to be determined in different cohorts and contexts. The synthesis provided here may be more defined by what is absent (figure 4). However, new innovations need to have a starting point, and now is an ideal opportunity to work collaboratively to cocreate a path forward for social prescribing and older adults.26
The field of social prescribing and older adults would benefit from expanding or including several new components within future studies. These include diversity of populations and community assets, different study designs, identifying and evaluating implementation factors, including behaviour change strategies or techniques (BCTs47) and data pathways. In particular, we need to understand what works for whom and under what circumstances, and some work has already started.10 Of note in our review, few studies reported consistently on factors such as ethnicity, education or socioeconomic status. A systematic review on social prescribing and newcomers reported the need for better descriptive information and the use of culturally and linguistically appropriate evaluation instruments.32 Furthermore, the range of social prescribing activities was narrow, mostly focused on physical or arts-based activities. As social prescribing can encompass a wide range of activities/support to address unmet needs, future studies could evaluate the effect on access to a wider range of community assets.
Beyond the ‘referral’ component of social prescribing are the actual activities undertaken, for which there is more supporting evidence. For example, systematic reviews summarise the benefits of social support and networks and older adults’ cognition,48 and arts-based interventions and older adults’ mental wellness.49 Based on a recent systematic review, findings were positive for physical activity interventions and social function, but no effect was found for physical activity and loneliness, social networks or social support.50 This may be in part because not all physical activity programmes are alike or because not all people enjoy group-based activities.51 For example, one study investigating people’s perspectives on group-based activities found that it could lead to stress for those who did not enjoy.51 These factors need to be considered in future social prescribing research and practice.
Study design is a key factor to consider in future trials of older adults and social prescribing. Larger and longer studies, preferably with a control or comparison group, would be essential elements in future projects. Within the included studies, two publications used the word ‘pilot’.41 43 Although pilot and feasibility studies are an important first step in developing an evidence base, they have limitations due to their small sample sizes.52 Other study designs to consider (beyond the typical randomised controlled trial) can assess the effectiveness or implementation of social prescribing, but to date these methods (eg, pragmatic trials,53 effectiveness-implementation hybrid design and/or stepped-wedge studies) have not been used in studies of older adults and social prescribing. Two other factors mentioned in the included studies to consider are to use mixed methods43 to capture and triangulate different types of data and studies or investigations from the societal perspective.42
There is a need to separate implementation details for the programme adoption and content at provider-level and person-level (eg, who makes referrals, does the person initiate the referral and start the community activity or resource, do they continue with it, etc) from the community-based interventions’ impact on health and social outcomes. From the included studies, two identified barriers were delay between making the referral and starting a programme,44 and lack of transportation41—both of which could impact on motivation. Reported reasons for not attending all of the available sessions were ‘illness, appointments or holidays’.46 A focus on implementation has started already, as outlined in the systematic review of facilitators and barriers to implementing social prescribing.16 We and others54 also noted low adherence rates in social prescribing studies. This may be due to numerous factors, including the practical barriers mentioned previously and other related factors such as stigma associated with some psychosocial programmes, people’s understanding and expectations for social prescribing and the limited nature of some programmes.55
In our review, only two studies reported on participants’ goals.40 42 However, literature highlights a gap between forming intentions (to start a new activity or behaviour) and behaviour change, also known as the intention–behaviour gap.56 Behaviour change can require goal setting and goal pursuit,57 in this case for both the older adults and provider. In our previous scoping review of reablement and BCTs,58 and concept mapping for implementing reablement,59 goal setting and pursuit were key concepts of model delivery. To date, only one systematic review (in a younger age group) focused on social prescribing and behaviour change,15 yet this may be one way to address the low rates of programme/study adherence. Adoption of behaviour change theory and strategies (for older people and providers) should be considered in future studies.
A motivating factor for social prescribing is the potential to reduce the impact on PCPs. In the current synthesis, there were differences in the findings for health resource use, although one study reported the benefits of social prescribing outweighed the associated costs.42 There is the need to work collaboratively on acceptable, effective, equitable and cost-effective innovations, while considering the well-being of health providers (ie, Quintuple Aim).60 As social prescribing continues to evolve, future studies could emphasise more team-based care, with the aim to reduce the workload on the GP and expand the older person’s circle of care. Social prescribing may provide a structured approach for PCPs to address social needs in primary care while providing access to resources, such as community link workers and non-medical community services. As per the work by Calderón-Larrañaga and colleagues,9 future work should determine if and how social prescribing impacts peoples’ lives. Furthermore, given the complexity of social prescribing, it is important to understand how the outcomes assessed are affected by the context in which social prescribing is delivered.
To date, both the UK and Australian GPs’ colleges commented on the potential for social prescribing in practice.61 62 In addition, the Royal College of General Practitioners (UK) have a partnership with Oxford University to provide three observatories on primary care and social prescribing data.63 Data science can support social prescribing; however, in our review, only two studies reported using routinely collected data.40 44 These are important strategies for people and places to consider when developing and testing social prescribing in a new setting.
Where to from here, when considering the current evidence on social prescribing and older adults? Minimising the consequences of unmet social needs is important and timely given the previous several years living in a pandemic. It has been almost two decades since the WHO convened the Commission on Social Determinants of Health, and longer since the first iterations of social prescribing emerged in the UK. Despite the small body of peer-reviewed evidence for social prescribing with older adults, it generates ideas and hypotheses. Future work should consider clinical–academic and/or community partnerships. Other considerations include developing a learning health system, defined by the Institute of Medicine as ‘health care system in which science, informatics, incentives, and culture are aligned for continuous improvement and innovation, with best practices seamlessly embedded in the care process, patients and families active participants in all elements, and new knowledge captured as an integral by-product of the care experience’64 p. 136. This may already be in place in the UK, as mentioned previously.63 Although it may be too soon to consider scaling up of social prescribing and older adults in places outside of the UK, Greenhalgh and Papoutsi65 suggest three different perspectives for moving innovations into practice at scale: implementation science, complexity science and social science. A framework or theory can help with next steps for social prescribing, and while each of these approaches could be adopted, given the complex nature of social prescribing, next steps should consider an integration of all three perspectives. Such as, implementation science may be useful to guide the reporting and evaluation of factors related to how social prescribing is adopted and sustained within a community setting, while complexity science supports pragmatic trial designs and flexibility (practice-based research). Finally, a social science perspective (eg, behaviour change and social support) has an important role for how a person may connect and feel connected to a social group or network.65
We note several limitations with this systematic review and the original studies. We were unable to identify many quantitative studies (and two were ‘pilot studies’41 43) specific to older adults and social prescribing. Pilot studies are inherently not hypothesis testing studies, and there is a risk of making inaccurate treatment effect assumptions. However, to our knowledge, this is the first systematic review focused on older adults with findings. As the number of studies are increasing, these results may change with new information. Although the included studies were at higher risk of bias due to study design and amount of missing information, these data are a call to create a roadmap for cocreating a future research and practice agenda for this content area.
Conclusion
Here we provide a synthesis of peer-reviewed evidence for social prescribing and older adults. Similar to other studies of younger populations,66 the evidence for social prescribing for older adults is limited in volume and methodology. However, it provides clues for how to move forward. Next steps should include development of a research and practice agenda that may include partnerships and a health learning system for social prescribing. Importantly, the community and people are in the best place to create the next steps.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
MCA gratefully acknowledges the support of the Canada Research Chairs Program.
References
Footnotes
Contributors All authors contributed to the study design and analysis and interpretation. AP and MCA conducted data collection. All authors approved the manuscript. MCA is the guarantor, and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.