Article Text

Abstract
Objectives Chronic conditions represent an important source of major health issues among Indigenous People. The same applies to those, who live off-reserve and in urban areas. However, very few healthcare services are considered culturally safe, resulting in some avoidance of the public healthcare system. Our goal was to review the literature on culturally safe practices available to urban Indigenous People who suffer from chronic diseases.
Design We conducted a scoping review to determine what culturally safe healthcare services are currently offered for the management of chronic conditions in urban Indigenous populations, to contribute to a tailored, holistic and safe space in mainstream healthcare systems.
Eligibility criteria Peer-reviewed original research articles had to be published by 27 October 2020, in English or French.
Information source: In October 2020, we searched five academic databases (EBSCO, PsycArticles, SocINDEX, MEDLINE and PsycINFO) and also reviewed grey literature and the websites of organisations or governments. The data were extracted and collected in an EXCEL spreadsheet. Two reviewers independently screened 326 titles and abstracts, followed by an independent evaluation of 48 full text articles. A total of 19 studies were included in this scoping review, as well as 5 websites/documents from the grey literature.
Results In total, 19 studies were included in our analysis. We found that Elders, family and the assistance of an interpreter are crucial elements to include to make urban Indigenous feel safe when they seek healthcare services. With this scoping review, we report interventions that are successful in terms of healthcare delivery for this population. Our findings provide insight on what services should be in place in mainstream healthcare settings to create a culturally safe experience for urban Indigenous People.
Conclusions In recent years, there appears to be a growing awareness of the need to provide culturally safe health services. This scoping review identified multiple strategies to promote cultural safety in this context, as well as barriers and facilitators to their implementation. These elements, which have been extensively documented in the literature, should be included in the chronic diseases management interventions to be developed by urban and primary care settings.
- health services research
- chronic disease
- health services, indigenous
- patient acceptance of health care
- urban health services
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- health services research
- chronic disease
- health services, indigenous
- patient acceptance of health care
- urban health services
Key points
What is already known on this topic
The number of Indigenous People living in urban areas is increasing.
Number of chronic diseases for Indigenous People is higher than in non-Indigenous people.
Urban Indigenous people suffer from the lack of culturally appropriate services for management of chronic diseases and this leads to poor health outcomes.
What this study adds
Interventions need to be culturally safe and are essential to prevent and manage chronic diseases among urban Indigenous People.
Patient-reported outcomes and experience measures increase when using culturally safe intervention in primary care.
How this study might affect research, practice and/or policy
Primary care clinicians should be adequately trained to provide culturally safe services to urban Indigenous People.
Decision-makers should provide human and financial resources to primary care clinics to enable them to use culturally safe interventions
Introduction
Indigenous people are more likely to live with chronic diseases, such as cardiovascular diseases and diabetes, than non-Indigenous people.1–5 Lack of adequate self-management programmes, support for chronic health conditions and difficulty in accessing care, often result in poor health and ultimately, death.1 5 6 These factors lead to higher proportion of overweight and obesity, higher smoking and less physical activity.2 7
Historically, colonialism has had an impact on health disparities and inequities that Indigenous People still experience to this day.8 As for racial discrimination, the link with one’s health status is documented and established as an important determinant of health.9 The concept of historical trauma refers to an intergenerational transmission of behaviours, unresolved grief and wounds, among other issues, that directly impact physical, emotional, mental and spiritual aspects of indigenous health.10 Morbidity, multimorbidity (co-occurrence of two or more unrelated chronic diseases) and mortality rates are significantly higher in Indigenous populations than in non-Indigenous ones.5 11
Over the last few years, an increasing number of Indigenous People have chosen to live in cities, as high as 55% in some urban areas, whether it is to study or for work.12 13 In addition, numbers are underestimated due to the difficulty in reaching Indigenous populations to complete censuses.14 Indigenous People in urban areas are more likely to experience food insecurity and poverty than Indigenous People living in rural areas or on-reserve, as well as compared with non-Indigenous people.15
This migration to urban centres leads to increased primary healthcare needs since it increases the number of persons attended to in healthcare services. However, services offered in urban areas are not consistently appropriate for Indigenous People who often feel forgotten by the healthcare system.16 Moreover, cases where Indigenous People are verbally abused by staff in hospitals are reported regularly.17 In a study led by Poitras et al,16 urban Indigenous participants admitted having reservations about consulting in the publicly funded healthcare services,18 fearing being bullied by hospital staff based on past experiences. Limited access to healthcare is an important social determinant of health.19 Moreover, gaps exist between quality of care provided to Indigenous People, as opposed to that of non-Indigenous.20 While some indigenous organisations, such as Native Friendship Centres in Canada, provide culturally safe health and community services, this is still not common in mainstream healthcare systems. In a recent study, Tremblay et al21 described the concept of cultural safety in healthcare as a transformative approach. Through culturally safe healthcare services, Indigenous patients can expect their core values to be recognised and respected through an equitable partnership between both parties. Cultural safety means that health professionals consider and acknowledge the needs, rights and culture of their Indigenous patients. Because the indigenous view of health refers to holistic wellness, including the spiritual, physical, mental and emotional spheres,22 it sometimes conflicts with western primary care.18 23 Therefore, healthcare providers must include both indigenous and western perspectives in their approach to providing culturally safe care for Indigenous People.23
Thus, with a growing proportion of Indigenous People living in urban areas, the implementation of culturally safe healthcare is essential. Recent calls for action, launched by different indigenous organisations,24 outline the necessity of delivering culturally safe services, as well as the need for a shift in the approach to healthcare. Moreover, it has been demonstrated that the first steps toward reducing inequities in healthcare services are to implement and test interventions.25 In this sense, the objective of this scoping review was to report on culturally safe interventions for the management of chronic diseases among urban Indigenous People. This scoping review sought to examine types of interventions, proposed key elements to deliver culturally safe care, as well as reported facilitators and barriers.
Methods
Patient and public involvement
Community members (Canapé and Bacon) were involved in the development of the research question, as implementing culturally safe interventions in chronic disease prevention is one of their priorities. They were also involved in identifying sources of information by targeting relevant websites and in the knowledge transfer plan by proposing efficient strategies to disseminate results to their communities.
Protocol
We developed a search protocol based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping reviews (PRISMA-ScR). We used the Population (P), Concept (C) and Context (C) approach, to define the search strategy and eligibility criteria (online supplemental table 1). The research question was ‘What are the culturally safe interventions (Concept) for the management of chronic diseases in primary care (Context), for Indigenous People living in an urban area (Population)?’ The PCC research question was discussed and validated by the authors. Specifically, we searched for culturally safe interventions in prevention and management of chronic diseases (mental or physical) of urban Indigenous people provided by primary healthcare professionals.
Supplemental material
Eligibility criteria
To be included in this study, articles had to present culturally safe interventions such as models of care, programmes, training for professionals, conceptual frameworks or any other actions leading to positive outcomes for Indigenous patients in the management of chronic diseases in primary care settings. Peer-reviewed original research articles had to be published by 27 October 2020, in English or French. All study designs were included except scoping and systematic reviews. We excluded articles for which we could not retrieve the full text through the Université de Sherbrooke library. From the perspective of a broader inclusion of sources, we searched for any grey literature related to our research question. Thus, two strategies were used to find additional data: (1) a customised Google search engine and (2) targeted websites. The inclusion criteria for the grey literature search were:
Most current version of the document (final or approved version).
Available in French or English.
Published by a government, professional association or an organisation representing Indigenous People.
Describing culturally appropriate methods to provide primary care in chronic diseases management.
Methods intended for urban Indigenous People.
Information sources and search
Five databases were searched: EBSCO, PsycArticles, SocINDEX, MEDLINE and PsycINFO. We used four main research concepts: ‘indigenous population’, ‘chronic disease’, ‘primary care’ and ‘cultural safety’. The exhaustive list of terms used for each database is available in online supplemental file 1. A manual search of the bibliography of relevant reviews identified by the initial searches was also performed. The results were imported into EndNote V.X7 (Clarivate Analytics, USA) for screening. For each internet search hit (5), we reviewed the first five pages by reading the titles and abstracts. The rationale behind the decision to screen the first five pages was to ensure that articles that were the most relevant would be captured. Moreover, by limiting to this number of pages, the articles to screen represented a reasonable number.26 The coauthors then created an Excel spreadsheet where all potentially relevant records were imported for further examination.
Selection of sources of evidence
To ensure a common understanding of the exclusion criteria, the two principal reviewers (T Vaillancourt and Boudreault) screened the first 10 articles independently and then discussed the results. Where there was insufficient or unclear information regarding the criteria, they discussed with a third reviewer (Poitras) to ensure common understanding. The exclusion criteria were then updated. Then, the two reviewers screened the titles and abstracts of the remaining articles in increments of 30 or 50, according to their schedule. The agreement rate of the reviewers was between 92% and 100%. There were no disagreements remaining after discussion.
Data charting process
The three reviewers (T Vaillancourt, Boudreault and Poitras) jointly developed an Excel data-charting form to select the variables to extract, and the Indigenous authors (Canapé and Bacon) of this paper participated in the discussion about the variables to be extracted from the texts. Two reviewers (T Vaillancourt and Boudreault) independently tested the chart by extracting data from two articles and having a discussion. Variables were added or removed according to this process. Each of the two reviewers performed the main extraction of half of the articles. Then, the second reviewer validated and improved the extraction of the other reviewer’s articles if necessary. A third reviewer (Poitras) validated the final extraction.
Data items
The final chart allowed the extraction of article characteristics (eg, country in which the study was done, year of publication, language, study design, goals) and population characteristics (eg, number of participants, age, sex ratio, type of chronic disease). Two reviewers (T Vaillancourt and Boudreault) also extracted data related to settings (context of primary care, number of clinics involved), interventions (type, tools used, name, cultural appropriateness, outcome measured), barriers and facilitators to implementation, and any other information deemed relevant. Moreover, they also performed a search of websites to inquire about any organisation, government, or other, that offers healthcare services for chronic diseases using a culturally safe approach.
Synthesis of results
The research team completed a narrative synthesis of the interventions described in the articles included. Based on the expertise and needs of urban indigenous community members, represented by the two Indigenous coauthors (Canapé and Bacon), we classified these interventions according to the following categories: relationships, cultural landmarks, spirituality/holistic health and access. When reported in the papers, the barriers and facilitators in the implementation of these interventions to inform future work were listed. Based on our research team’s expertise, we also explored the data from the perspective of Indigenous People and healthcare professionals to identify differences or similarities.
Results
Selection of sources of evidence
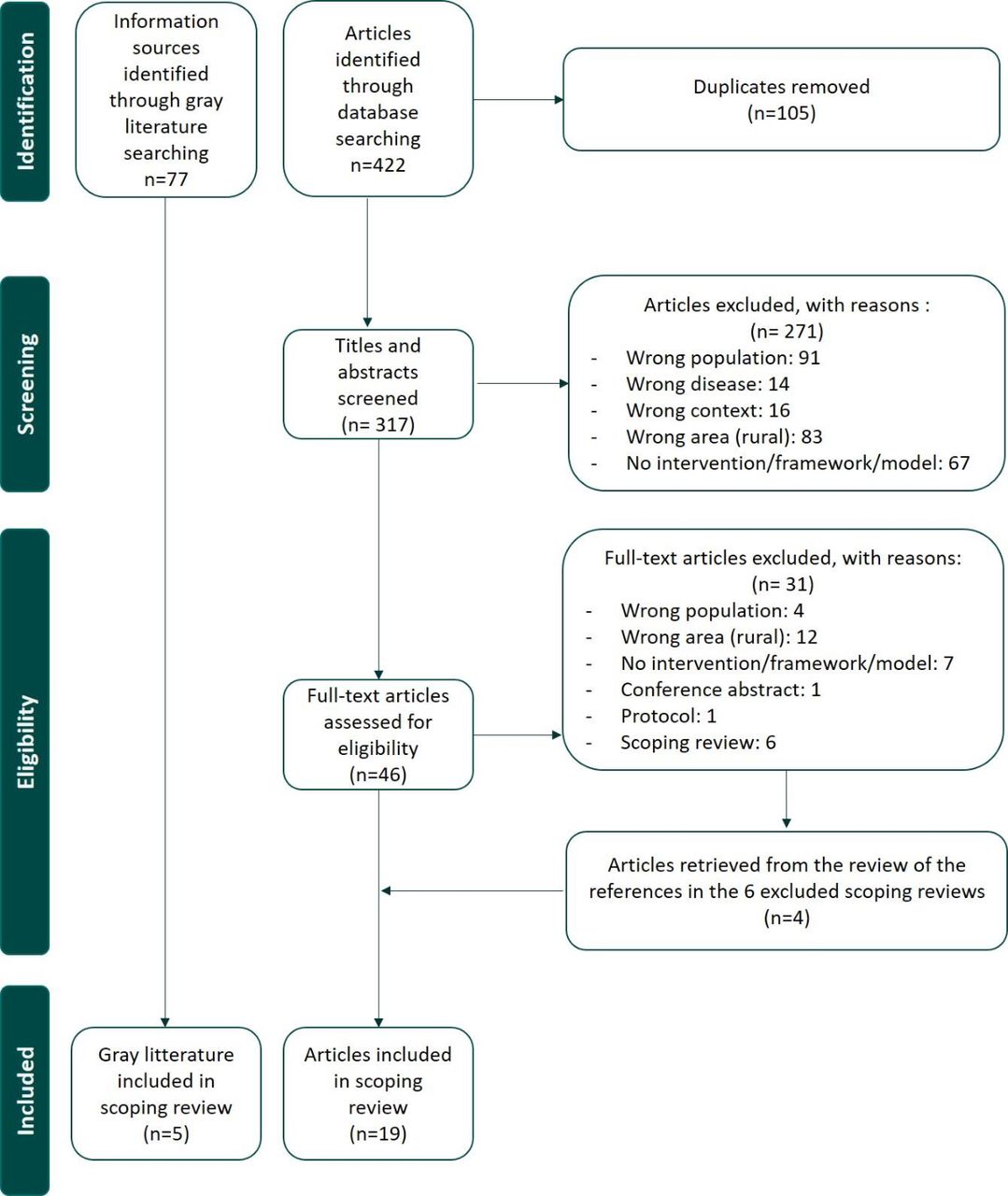
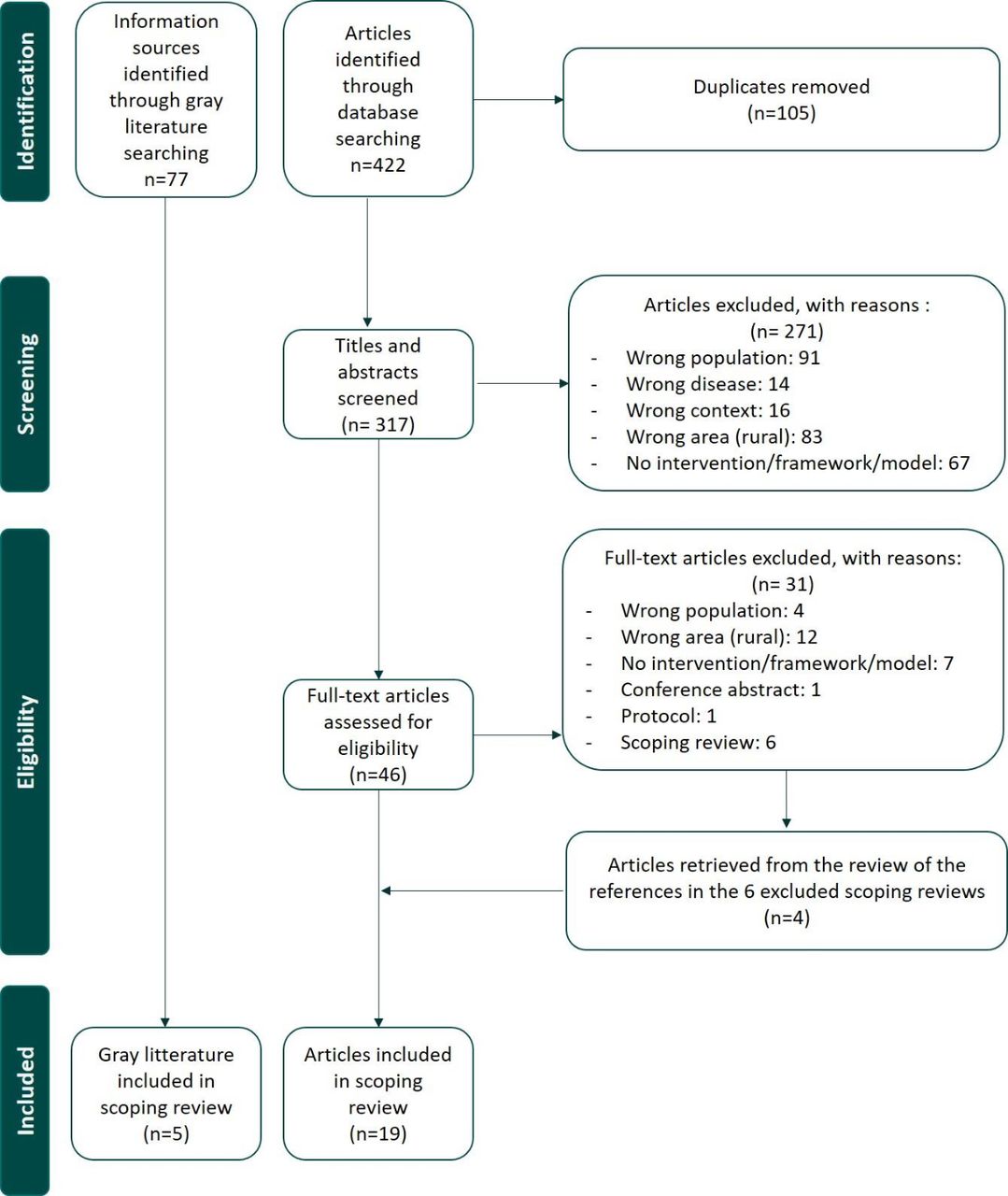
The research team conducted the search in October 2020 and assessed 422 articles for eligibility. One hundred and five duplicates were removed from the list and the two independent reviewers forwarded 317 articles to titles and abstracts screening. After an independent screening of titles and abstracts by the reviewers, 46 articles were selected for full-text reading. Of these, 31 did not meet our inclusion criteria and were excluded. The reviewers excluded scoping and systematic reviews but screened their references to identify potentially relevant articles. Thus, four additional articles were added making a final total of 19 articles that were included for data extraction. For the grey literature internet search, 77 potentially relevant websites/documents were found among the first five pages of results. After screening, five were kept for data extraction. Figure 1 presents the flow chart for the selection of sources of evidence.
{kind=link}
Flow chart for the selection of sources of evidence.
Characteristics of the sources of evidence
All articles that were included in this scoping review had received ethic approval. All the included articles were published after 2008 and the number of articles increased with the year of publication (2008–2010 n=3; 2011–2013 n=1; 2014–2016 n=6; 2017–2019 n=9). From these studies, five (26%) used a qualitative design, seven (37%) a mixed-methods design, two (11%) were cohort studies, two (11%) were randomised control trials and one (5%) was a pilot study. Most studies (n=14; 74%) were conducted in Australia and New Zealand (online supplemental figure 1a), and interventions were mainly targeted to Torres Islanders and Aboriginal Australians (5/16; 31%) or Maori and Pacific Peoples (5/16; 38%). Most studies explored diabetes issues (n=9/15; 60%) and were single disease oriented (68%) (online supplemental figure 1b). Characteristics of included studies such as place of origin, study design, population and setting are presented in table 1. As for websites, we aimed to retrieve data from different organisations that provide culturally safe healthcare to urban Indigenous People. We identified five websites describing culturally safe interventions for chronic diseases of urban Indigenous Populations. More than half were government sites (3/5) and two were private or community organisation sites. Four referred to Canadian entities and one to Australian ones.
Characteristics of the studies included
Results of individual sources of evidence
The studies and websites reported interventions, for the most part, in the form of programmes (n=8, 1 website), models of care (n=3, 2 websites),27–29 programmes of care (n=5, 1 website),30–34 training for clinicians (n=3)19 35 36 or patients (n=3),36–38 and frameworks guiding the delivery of culturally safe care (n=1, 1 website). They were all implemented in clinical settings to provide culturally safe care for Indigenous populations. The interventions reported involved mostly nurses (n=14),19 27–29 32–41 social workers or community workers (n=11),19 27 28 30 31 35 37–40 42 physicians (n=9),19 28 29 32–35 41 43 coordinators (n=3),27 35 42 administrative staff (n=4),32 34 35 40 dietitians (n=4),27 36 38 39 managers (n=4),30 35 38 42 pharmacists (n=2),19 30 Elders (n=4),19 29 32 34 psychologists/psychiatrists (n=5).27 29 32 34 39 All the interventions presented on the websites mentioned the involvement of interprofessional teams. Table 2 presents culturally safe interventions.
Culturally safe interventions for the prevention and management of chronic diseases
Synthesis of results
To enhance cultural safety of practices in chronic disease management in primary care, several types of interventions were used. First, educational interventions aimed at patients were reported such as the ‘DEFEND’ programme focusing on diabetes and its complications as described by Hotu et al37 or the Te Hauora O Ngati Rarua programme, a 6-week course about wellness and self-management education implemented by Janssen and Nelson.38 Other educational interventions were aimed at clinicians, such as ‘My Health Story’, which is a training programme composed of a toolkit and a booklet reported by Battersby et al.35 Some were intended for both patients and clinicians, such as the ‘Curriculum’ detailed in the Sinclair Ka’imi et al’s study.44 Some implemented models of care, such as He Pikinga Waiora28 that aims to increase access to podiatrists, provide frequent follow-ups with a nurse and give financial support to Indigenous patients. Several studies reported enhanced practices for clinicians following the intervention. For example, recognising culture as an interactive process, focusing on patient’s context and priorities, securing more time for interaction with patients43 and promoting collaborative work as solutions to enhance practice.42
All the interventions had high acceptability among Indigenous participants and, although some did not have significant results on biological target values (eg, weight, high-density lipoprotein level), they all had positive results on patient-reported outcomes (PROMs) or patient-reported experience measures (PREMs), which align with the indigenous vision of health. Feeling respected and supported was the most common PREM reported in the studies included.27 28 32 35 36 39 In the Battersby et al’s study, a training and booklet for self-management of chronic conditions was used by healthcare professionals and patients reported feeling supported, respected and understood, and able to discuss their concerns for the first time.35 Culturally safe interventions in care also influenced PROMs, as reported by Askew et al, who used a home-based case management model that led to improvements in the mental and emotional health of Indigenous patients.27 Battersby et al reported decreased stress and anxiety levels, improved social support and ability to manage prescription payments, and the ability to maintain a healthy diet and level of exercise.35 The inclusion of Elders in the direct care of Indigenous patients reported in both of the studies by Hadjipavlou et al, led to a decrease in suicidal thoughts and depressive symptoms among the Indigenous participants.32 34
Multiple strategies for cultural safety were employed to promote the success of the interventions presented by the authors of the articles selected for this scoping review. They are classified in five categories and presented in table 3. Briefly, the first category, relationships, refers to strategies that promote the development of trusting relationships between healthcare providers and Indigenous People such as the inclusion of the family in care.28 29 33 36 38 42 The second category, cultural landmarks, refers to concrete elements of indigenous culture that should be included in environments where Indigenous patients receive care, such as the inclusion of indigenous artwork in clinics.30 Spirituality and holistic health, the third category, proposes strategies to provide more holistic care, and to consider the four dimensions of indigenous well-being (physical, emotional, mental and spiritual), including the use of prayers and songs.38 Access to healthcare, the last category, lists strategies to increase access to care of Indigenous patients such as offering transportation to clinics.33 37
Strategies identified to promote cultural safety in chronic disease prevention and promotion
While some practices tend to be facilitating in building good relationships and allowing cultural safety in the delivery of care, others can hamper it. Table 4 presents barriers and facilitators for Indigenous patients living in urban areas, for clinicians and for both, in the implementation of culturally safe interventions. According to Indigenous patients, components such as the absence of a holistic approach42 43 as well as discrimination31, jeopardised effective healthcare. For clinicians, one of the reported barriers was the lack of support from government42, managers and peers.35 From both the perspectives of clinicians and patients, language37 42 and medical jargon hindered care.43 The only facilitator reported by both clinicians and patients were the recognition of culture.38 42 43 In addition, patients are favourable to the use of community-based activities,40 44 while clinicians identified the reduction of caseloads36 42 and a demedicalised approach31 as facilitators. We observed no differences in intervention characteristics when we compared studies by country or population.
Barriers and facilitators in the implementation of culturally safe interventions
Discussion
In this scoping review, the research team identified 19 studies, published before 27 October 2020, and 5 websites describing culturally safe interventions for Indigenous populations. There were several culturally safe interventions for chronic disease management in urban Indigenous populations that were implemented in primary care organisations. The interventions described took the form of educational programmes, models and programme of care, and frameworks, mostly targeted diabetes, were largely implemented in Australia or New Zealand, and involved nurses, physicians and social workers more than other professionals.
One of the findings of this scoping review is that even though chronic diseases in the form of multimorbidity are constantly increasing,45 the vast majority of the culturally safe interventions studied targeted a single disease, and few incorporated a global approach to care or multiple chronic conditions. However, the literature shows that a single disease approach to care provides fragmented, incomplete and even ineffective care46 47 and that integrated care brings positive outcomes for patients.48 49 Furthermore, as Indigenous patients are experiencing difficulties in navigating Western healthcare services, a single disease approach brings even more barriers. Indeed, with a global approach to care, the number of healthcare professionals involved in a patient’s trajectory is limited and allows Indigenous patients to build trusting relationships that are essential to cultural safety of care. Also, a single disease approach conflicts with indigenous cultural values related to holistic health.
In this scoping review, several interventions were in the form of educational interventions aimed not only at patients but also at healthcare professionals that lack training in cultural safety. This observation is in line with the literature.50 51 One of the key aspects of improving cultural safety in the delivery of care and services in primary care is the development of cultural competency of caregivers.52–54 Cultural awareness and training of healthcare professionals is the cornerstone of this process. By being more aware of Indigenous people’s history and culture, healthcare professionals will be able to include more easily elements of cultural safety in their practice, such as the inclusion of family, the use of appropriate visual aids, or the consideration of spirituality. This cultural competency increases the equity and quality of delivered care but also reduces broader healthcare inequities between Indigenous and non-Indigenous people.55 56 This is also consistent with the Etuaptmumk (two-eyed seeing) framework,57 which aims to use both Western and traditional strengths and knowledge so that the patient benefits from the advantages of each.
This scoping review also strengthened the importance of Elders as traditional healers and guides for Indigenous People to maintain wellness and balance between the different spheres of holistic health. Elders’ experiential knowledge is a valid and legitimate source of evidence in indigenous culture.58 59 They play an important part in implementing culturally safe practices. In Canada and even more in the Province of Quebec, Elders have very little presence in public primary care. In addition, they generally live in communities, and few are present in urban areas. Thus, access to their teachings and holistic care is limited in urban areas. Indigenous People must travel to their communities to access this traditional care. As urban Ondigenous populations are growing and getting younger, there is a need to think about ways to increase access to Elders. As identified in this scoping review, the active role of Elders in chronic disease prevention and promotion is a key strategy in promoting cultural safety. Although Elders are increasingly involved in primary healthcare delivery in some countries, they are not yet recognised as legitimate providers, at least in Canada.34 This lack of recognition reduces their ability to provide culturally safe and indigenous-recognised health services in urban primary care. Government authorities could legislate this and recognise Elders as healthcare professionals in the same manner as a nurse or social worker. To facilitate this recognition, longitudinal studies are needed to explore the outcomes of Elders as primary care providers to support this innovative proposal with decision-makers.
Finally, we did not observe any real differences between populations or countries where the studies were conducted. Regardless of their origin, the basic principles of cultural safety are the same whether care is provided in urban or non-urban settings. On the other hand, despite similarities in historic and social determinants of health of Indigenous populations from Canada, Australia, New-Zealand and the USA,60 the extent of the literature differs between these countries. This scoping review highlighted the lack of literature on contributions by Canada to implementing culturally safe interventions for Indigenous People living with chronic diseases in urban settings. Canada is still in the early stages of indigenous research in primary care. Indeed, Canada’s Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (TCPS 2), included for the first time a chapter on research involving First Nations, Inuit and Metis peoples in 2010. However, the Canadian Institutes of Health Research has committed since 2017 to investing a minimum of 4.6% of its annual budget on research aimed at improving the health of Indigenous People.61
Our article provides practical tools for family medicine and community health professionals who provide urban primary care to Indigenous People. This article provides concrete examples of interventions to improve cultural safety in care. It offers a starting point for thinking about how to implement culturally safe practices. PRISMA-ScR guidelines were used to report the scoping review findings and the study selection process was rigorous. Due to time constraints, the internet search was limited to the first five pages of results and therefore some sources of information may have been missed. The criteria of the search strategy are a limitation of our study. The selection of the search engine (EBSCO) and databases, as well as the research terms certainly influenced the list of articles obtained and again some data may have been missed. Finally, as indigenous people transmit their knowledge orally, we could had missed some culturally safe interventions in our research.
Conclusion
This scoping review highlights the development and implementation of culturally safe interventions for chronic disease prevention and management among urban Indigenous People. The studies reviewed identified multiple and varied strategies to promote cultural safety in this context, as well as barriers and facilitators to their implementation. However, the study found that the interventions promoted more chronic disease management in favour of a holistic approach. In addition, our work also shows that there is a lack of support for the development of professionals’ skills. Finally, the presence of an Elder is an essential condition in the context of chronic diseases that promotes recovery and global health. These elements, which are abundantly listed in the literature, could be included in the chronic disease management interventions that will be developed by urban and primary care settings.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Meve_Poitras, @chaire_pposp
Contributors M-EP, AC, KB and SH conceived of the presented idea. M-EP directed the study and is the guarantor and accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish. VTV and AB performed the review and wrote the draft of the manuscript. M-EP and SH revised the manuscript. All authors discussed the results and commented on the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.