Article Text

Abstract
Objective Because of their increased interaction with patients, healthcare workers (HCWs) face greater vulnerability to COVID-19 exposure than the general population. We examined prevalence and correlates of ever COVID-19 diagnosis and vaccine uncertainty among HCWs.
Design Cross-sectional data from the Household Pulse Survey (HPS) conducted during July to October 2021.
Setting HPS is designed to yield representative estimates of the US population aged ≥18 years nationally, by state and across selected metropolitan areas.
Participants Our primary analytical sample was adult HCWs in the New York Metropolitan area (n=555), with HCWs defined as individuals who reported working in a ‘Hospital’; ‘Nursing and residential healthcare facility’; ‘Pharmacy’ or ‘Ambulatory healthcare setting’. In the entire national sample, n=25 909 HCWs completed the survey. Descriptive analyses were performed with HCW data from the New York Metropolitan area, the original epicentre of the pandemic. Multivariable logistic regression analyses were performed on pooled national HCW data to explore how HCW COVID-19-related experiences, perceptions and behaviours varied as a function of broader geographic, clinical and sociodemographic characteristics.
Results Of HCWs surveyed in the New York Metropolitan area, 92.3% reported being fully vaccinated, and 20.9% had ever been diagnosed of COVID-19. Of the subset of HCWs in the New York Metropolitan area not yet fully vaccinated, 41.8% were vaccine unsure, 4.5% planned to get vaccinated for the first time soon, 1.6% had got their first dose but were not planning to receive the remaining dose, while 52.1% had got their first dose and planned to receive the remaining dose. Within pooled multivariable analysis of the national HCW sample, personnel in nursing/residential facilities were less likely to be fully vaccinated (adjusted OR, AOR 0.79, 95% CI 0.63 to 0.98) and more likely to report ever COVID-19 diagnosis (AOR 1.35, 95% CI 1.13 to 1.62), than those working in hospitals. Of HCWs not yet vaccinated nationally, vaccine-unsure individuals were more likely to be White and work in pharmacies, whereas vaccine-accepting individuals were more likely to be employed by non-profit organisations and work in ambulatory care facilities. Virtually no HCW was outrightly vaccine-averse, only unsure.
Conclusions Differences in vaccination coverage existed by individual HCW characteristics and healthcare operational settings. Targeted efforts are needed to increase vaccination coverage.
- COVID-19
- Vaccination Refusal
- Health Facilities
- Preventive Medicine
Data availability statement
Data are available in a public, open access repository. US Census Bureau. Measuring Social and Economic Impacts during the Coronavirus Pandemic. Available at https://www.census.gov/programs-surveys/household-pulse-survey.html. Accessed on 31 December 2021.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
As a result of their increased interaction with patients, healthcare workers face greater vulnerability and higher risk to COVID-19 exposure than the general population.
What this study adds
COVID-19 exposure and vaccination status among healthcare workers varied by type of healthcare facility and various individual-level characteristics. Of healthcare workers surveyed in the New York Metropolitan area during 21 July 2021 to 11 October 2021, 92.3% reported being fully vaccinated, and 20.9% had ever been diagnosed of COVID-19. Personnel in nursing/residential facilities were less likely to be fully vaccinated and more likely to report ever COVID-19 diagnosis, than those working in hospitals. Of healthcare workers not yet vaccinated, vaccine-unsure individuals were more likely to be white and work in pharmacies, whereas vaccine-accepting individuals were more likely to be employed by non-profit organisations and work in ambulatory care facilities.
How this study might affect research, practice, or policy
Enhanced and sustained efforts are needed to increase protections for healthcare workers in diverse settings, including through use of personal protective equipment, increased infection control education and training, and expanded vaccine coverage, including booster doses.
Introduction
Healthcare workers (HCWs) have played and continue to play a key part in preventing and controlling COVID-19 spread through health and vaccine educational activities, direct patient care and support of contact tracing and disease surveillance. Because of their repeated and close interactions with patients, HCWs may have a higher risk of contracting COVID-19 than the general population.1 This risk may vary based on community disease burden, disease severity and healthcare facility type.2 3 These differences in risk exposure may influence perceived susceptibility to COVID-19 and vaccine receptivity.
Most HCWs in New York are now vaccinated but intensified efforts are needed to target and extend coverage to the unvaccinated.4 While small, the unvaccinated segment is by no means trivial. HCWs are trusted sources of health information and their attitudes and perceptions can influence patient behaviours and social norms.5 As COVID-19 vaccine hesitant individuals are either vaccine averse (ie, will refuse any COVID-19 vaccine) or vaccine unsure (ie, are ambivalent or have some reservations about receiving any COVID-19 vaccine), targeted vaccination campaigns will need insights into characteristics of both groups of individuals to craft effective public health messages and boost efficiency of outreach efforts.6 7 Much of the research on HCW vaccine confidence were conducted before or shortly after COVID-19 vaccines became available through Emergency Use Authorisation and may no longer reflect the current landscape.8–16 Some of these studies have been further limited by their lack of generalisability and their narrow focus on clinicians even though non-clinical staff can also expose others if infected.4 8 9 16 17 Up to date data are needed to characterise the HCW subpopulations at highest risk for SARS-CoV-2 infection for whom vaccines (including boosters) would particularly be beneficial. Furthermore, a better understanding of factors associated with vaccine hesitancy among unvaccinated HCWs could help inform tailored public health planning, programmes and policy aimed at increasing vaccine uptake.
To better characterise weak points in SARS-CoV-2 exposure and vaccine attitudes by role of personnel and type of healthcare facility within the New York Metropolitan area, the objective of this study was to measure prevalence, correlates and disparities in self-reported ever COVID-19 diagnosis and full vaccination status.
Methods
Data source
Analysed data were from the Household Pulse Survey (HPS), a COVID-19 surveillance system designed to yield representative estimates for the US overall, all 50 US states and Washington, DC, as well as selected metropolitan areas. We largely focused on the New York Metropolitan Area for descriptive analyses given that New York City (NYC) was the original epicentre of the pandemic in the USA and still has a higher incidence rate than the national average.18–21 We also drew on pooled national HPS data within multivariable analyses to explore how HCW COVID-19-related experiences, perceptions and behaviours varied as a function of broader geographic, clinical and sociodemographic characteristics.
HPS is a recurring, online survey of the US population aged ≥18 years.22 Conducted by the US Census Bureau, this survey is designed to yield representative estimates of persons aged ≥18 years nationally, by state and across selected metropolitan areas. HPS utilises the Census Bureau’s Master Address File as the source of sampled housing units. The sample design was a systematic sample of all eligible housing units, with adjustments applied to the sampling intervals to select a large enough sample to create state level estimates and estimates for the top 15 metropolitan statistical areas. Survey invitations are distributed to eligible participants via email and SMS, and data collection is done using Qualtrics. We analysed six survey cycles, ‘HPS week 34’ (21 July 2021–2 August 2021) through ‘HPS week 39’ (29 September 2021–11 October 2021). The study period was approximately a year and half into the COVID-19 pandemic in the USA. This period was characterised by a resurgence of new COVID-19 diagnoses following the first wave of cases. During the study period, July 2021–October 2021, daily number of cases nationally peaked at 3519 new cases/day in mid-September 2021, with NYC making a substantial contribution to recorded new cases.20 23 Our main geographical unit for descriptive analysis was the New York Metropolitan area (‘NY-NJ-PA Metro Area’), which comprises 10 counties in New York State (covering the five boroughs of NYC, three counties in the lower Hudson Valley, and the two counties of Long Island); 12 counties in New Jersey and 1 county in Pennsylvania.24 Of participants from this Tri-state Metro Area in our sample, 62.3% came from New York State.
The indicated study population for our analyses was individuals who reported physically working in a healthcare setting during the pandemic. Survey participants were asked ‘Since 1 January 2021, which best describes the primary location/setting where you worked or volunteered outside your home?’ Those who selected any of the following answers were classified as working in a healthcare setting: ‘Hospital’; ‘Nursing and residential healthcare facility’; ‘Pharmacy’; ‘Ambulatory healthcare (eg, doctor, dentist or mental health specialist office, outpatient facility, medical and diagnostic laboratory, home healthcare)’. This question was framed to capture past-year, on-site work well into the COVID-19 pandemic, which could conceivably have been different from work before or at the start of the pandemic (eg, lay-offs or telework). Using ‘1 January 2021’ as a reference point (rather than 1 January 2020) was therefore a means of reducing the potential for misclassification of employment status/setting by capturing respondents’ more recent work situation and by reducing the recall window. Of the 442 741 individuals across the USA who completed the six cycles of HPS conducted during July to October, 2021, those identifying as HCWs nationwide numbered 25 909. Within the New York Metropolitan area, the number of adults identifying as HCWs was n=555.
Measures
Self-reported ever COVID-19 diagnosis: This was defined as a response of ‘Yes’ to the question ‘Has a doctor or other health care provider ever told you that you have COVID-19?’
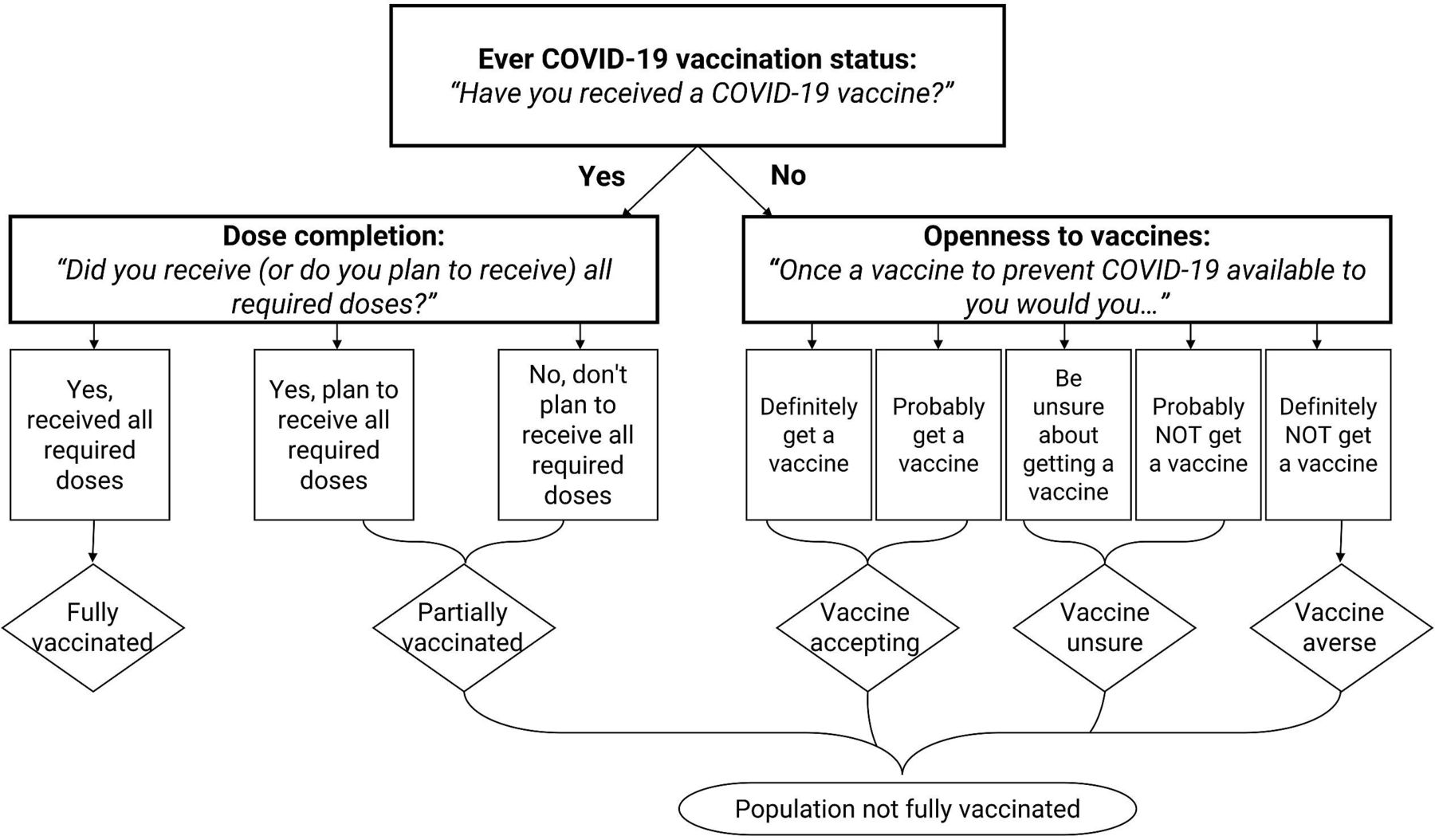
Full COVID-19 vaccination status : To determine vaccination status, two questions were asked. Q1: ‘Have you received a COVID-19 vaccine?’ [Response options: ‘Yes’ or ‘No’]; Q2: ‘Did you receive (or do you plan to receive) all required doses?‘[Response options: ‘Yes, received all required doses’, ‘Yes, plan to receive all required doses’, or ‘No, don't plan to receive all required doses’]. Those who answered ‘Yes’ to Q1 and ‘Yes, received all required doses’ to Q2, were classified as being fully vaccinated (figure 1).

Definition of various COVID-19 vaccine statuses and dispositions, Household Pulse Survey, 21 July 2021 to 11 October 2021.
Openness to COVID-19 vaccine among the unvaccinated: Among only those who had never received a single dose of COVID-19 vaccine, the survey asked ‘Once a vaccine to prevent COVID-19 available to you would you…’ 1) ‘Definitely get a vaccine’; ‘Probably get a vaccine’; ‘Be unsure about getting a vaccine’; ‘Probably NOT get a vaccine’; ‘Definitely NOT get a vaccine.’ We used participants’ responses to categorise them as vaccine averse (a ‘definitely not’ response), vaccine unsure (a ‘probably not’ or an ‘unsure’ response) or vaccine accepting (‘Definitely get a vaccine’ or ‘Probably get a vaccine’).
Key explanatory variables: These included sociodemographic characteristics like gender, age group, employer (government, private, non-profit organisation, self-employed/family business, other), household type (ie, multiple, or single adult household with or without children) and dwelling (single or multiunit dwelling). As the survey did not collect information on type of role (eg, clinical vs support staff), we used highest educational attainment as a proxy for role.
Statistical analyses
Prevalence estimates with corresponding 95% CIs, for ever COVID-19 diagnosis and full vaccination status, were computed for HCWs, overall and by healthcare setting, highest educational attainment, employer, household structure, type of housing, number of people living with respondent in the household, race/ethnicity, gender, age, annual household income, self-rated financial difficulty and health insurance type. Prevalence estimates with relative SEs (RSEs) ≥40% were deemed statistically unreliable. We compared HCWs in the New York metropolitan area vs the rest of the USA in relation to main study endpoints using two tailed χ2 tests. Using pooled data of all HCWs nationwide to increase sample size (n=25 909), two logistic regression models were fitted to evaluate binary indicators of COVID-19 ever diagnosis and full vaccination status as functions of key explanatory variables and control covariates. A third binary logistic regression model was fitted among all HCWs nationwide who had not yet received a single dose of the COVID-19 vaccine (n=1872) to evaluate correlates of vaccine uncertainty. Our null hypothesis was that these indicators had no association with key explanatory variables. A two-sided alpha of 0.05 was used to determine statistical significance. Data were weighted to account for the complex survey design and yield representative estimates. Analyses were performed with Stata version 15.
Results
In total, 49.7% of HCWs in the New York Metropolitan area worked in a hospital, 56.1% reported that their employer was a private organisation, 38.4% were white and 28.0% reported having a doctoral/professional/master’s degree. Other characteristics are presented in table 1.
Sociodemographic characteristics and percentage ever diagnosed of COVID-19 as well as the percentage fully vaccinated among healthcare workers in the New York (NY) Metropolitan area (n=555), Household Pulse Survey, 21 July 2021 to 11 October 2021
Ever COVID-19 diagnosis among HCWs in the new York Metropolitan area and nationally
Prevalence of self-reported ever COVID-19 diagnosis among all HCWs was 20.9% (95% CI 14.3% to 27.5%) in the New York Metropolitan area and did not differ significantly from the rest of the country (19.8%, p=0.736). Within pooled analysis nationwide, the odds of ever COVID-19 diagnosis were higher among HCWs in nursing/residential facilities than hospitals (AOR)=1.35, 95% CI 1.13 to 1.62) and among those partially vaccinated (AOR 1.82, 95% CI 1.36 to 2.43) or unvaccinated (AOR 2.65, 95% CI 2.05 to 3.42) than fully vaccinated. Odds of ever COVID-19 diagnosis were lower among those working in the non-profit than the private sector (AOR 0.82, 95% CI 0.69 to 0.97) and those aged ≥65 years than 18–24 years (AOR 0.57, 95% CI 0.36 to 0.91). Compared with HCWs who had a doctoral/professional/master’s degree, the odds of ever COVID-19 diagnosis were higher among those with an associate degree (AOR 1.49, 95% CI 1.23 to 1.81), some college but no diploma (AOR 1.44, 95% CI 1.19 to 1.73) and <high school (AOR 2.51, 95% CI 1.35 to 4.66). HCWs ever diagnosed of COVID-19 were more likely to be Hispanic (AOR 1.36, 95% CI 1.09 to 1.71) or black (AOR 1.27, 95% CI 1.03 to 1.57) than White.
Vaccination profile of HCWs in the New York Metropolitan area and nationally
Of HCWs in the New York Metropolitan area, 92.3% were fully vaccinated, significantly higher than the rest of the country. (86.4%, p=0.005). This difference was driven by significantly higher vaccination rates for nursing personnel in the New York Metropolitan area than the rest of the nation (93.0% vs 80.3%, p=0.010). No significant differences existed for other settings. Pooled multivariable logistic regression analysis revealed that the odds of being fully vaccinated were significantly lower among HCWs in nursing facilities than hospitals (AOR 0.79, 95% CI 0.63 to 0.98) (table 2). Compared with HCWs with a doctoral/professional/master’s degree, the odds of being fully vaccinated decreased with decreasing education as follows: college degree (AOR 0.68, 95% CI 0.54 to 0.84), associate degree (AOR 0.35, 95% CI 0.28 to 0.44), some college but no diploma (AOR 0.33, 95% CI 0.26 to 0.41), high school diploma (AOR 0.26, 95% CI 0.19 to 0.35) and <high school (AOR 0.37, 95% CI 0.20 to 0.67). HCWs who worked for non-profit organisations reported 50% higher odds of being fully vaccinated than those in the private sector (AOR 1.50, 95% CI 1.21 to 1.85). Differences also existed by race/ethnicity, age, US Census region and household characteristics (table 2). For example, the odds of being fully vaccinated among non-Hispanic Asians were two-fold higher compared with non-Hispanic Whites (AOR 2.19, 95% CI 1.30 to 3.67). Even though older adults aged ≥65 years had 43% lower odds of being ever diagnosed of COVID-19 compared with younger adults aged 18–24 years (AOR 0.57, 95% CI 0.36 to 0.91), no significant differences existed between the extremes of age in the odds of being fully vaccinated. By US Census region, whereas no significant differences existed in the adjusted odds of ever COVID-19 diagnosis among HCWs, the adjusted odds of being fully vaccinated were significantly lower among those in the South (AOR 0.58, 95% CI 0.45 to 0.75) and Midwest (AOR 0.59, 95% CI 0.45 to 0.77) compared with the Northeast.
Adjusted ORs with corresponding 95% CIs for factors associated with ever COVID-19 diagnosis and being fully vaccinated among all healthcare workers in the US
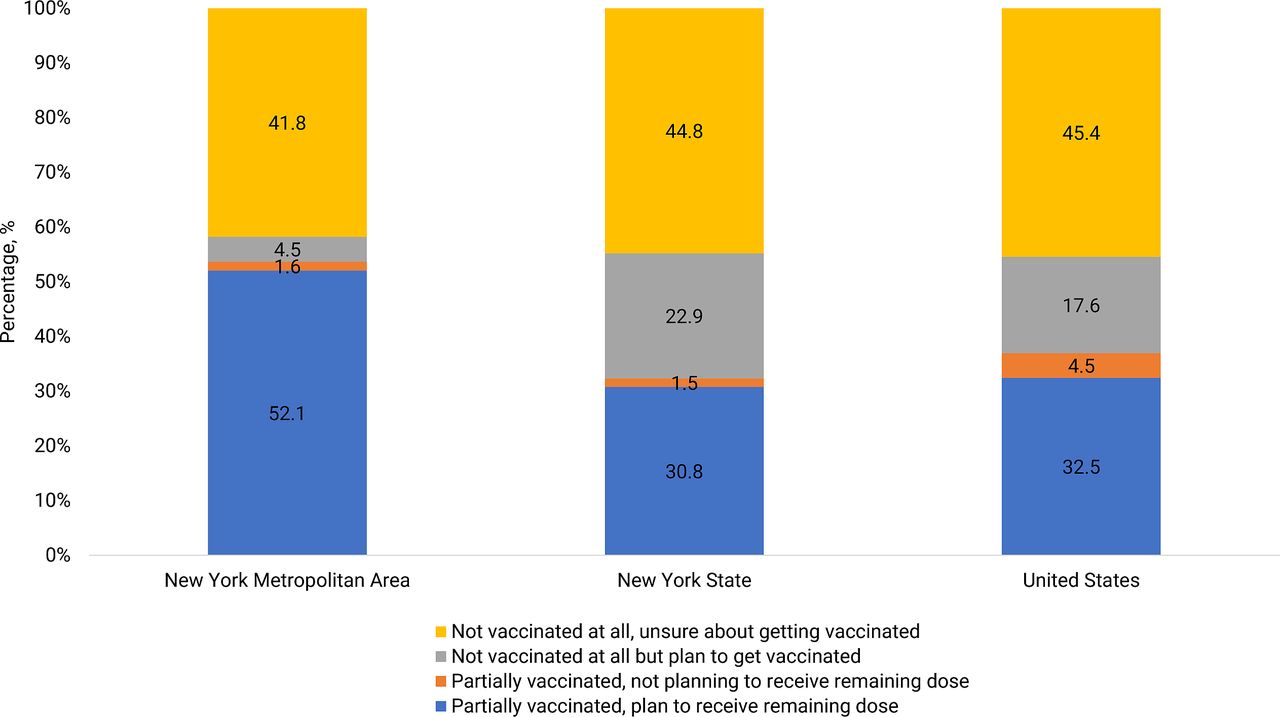
Of the subset of HCWs in the New York Metropolitan area not fully vaccinated (inclusive of partially vaccinated and unvaccinated individuals), 41.8% were vaccine unsure, 4.5% planned to get vaccinated for the first time soon, 1.6% had received their first dose but were not planning to receive the remaining dose, while 52.1% had received their first dose and planned to receive the remaining dose (figure 2). Virtually no HCW reported being vaccine averse. Pooled multivariable analysis of those who had never received a single vaccine dose revealed that the odds of being vaccine-unsure were higher among those aged 45–64 and ≥65 years than 18–24 years and those living in mobile housing or in a one-family house detached from any other house, when compared with those living in a multiunit apartment complex (table 3). Compared with HCWs within hospital settings, odds of being vaccine-unsure were higher among those working in pharmacies (AOR 3.67, 95% CI 1.05 to 12.82) but lower among those working in ambulatory centres (AOR 0.50, 95% CI 0.28 to 0.89). The odds of being vaccine-unsure were also lower among those working for non-profit organisations than the private sector (AOR 0.46, 95% CI 0.24to 0.87) and among blacks than whites (AOR 0.33, 95% CI 0.17 to 0.67).
{kind=link}
{kind=link}
Perceptions and attitudes towards COVID-19 vaccines among the subset of healthcare workers not yet fully vaccinated, by geographical location (overall n=2606), Household Pulse Survey, 21 July 2021 to 11 October 2021.
Adjusted ORs with corresponding 95% CIs for factors associated with vaccine uncertainty among unvaccinated healthcare workers in the U.S.
Discussion
Of HCWs surveyed in the New York Metropolitan area during 21 July 2021 to 11 October 2021, we found that 92.3% reported being fully vaccinated, and 20.9% had ever been diagnosed of COVID-19. Like other studies, our analysis of the national HCW sample revealed that nurses, individuals living in the South or Midwest, and those with lower education, all were less likely to be fully vaccinated, whereas Asians were more likely to be fully vaccinated.10 14 Our contribution to the growing body of evidence is that vaccine-unsure HCWs are more likely to be white, work in pharmacies and live in single unit housing, whereas vaccine-accepting HCWs were more likely to be employed by non-profit organisations, and work in ambulatory care facilities. The increased likelihood of vaccine uncertainty among HCWs in pharmacies and nursing facilities is concerning because of their frequent interactions with potentially contagious, unscreened individuals within their work environment.1 17 25 26 Underlying reasons for vaccine uncertainty among HCWs, including pharmacists, identified in previous studies have included the perception that pharmaceutical companies may be hiding some important information on COVID-19 to promote the sale of their products, doubts on the reliability and trustworthiness on the COVID-19 vaccine safety and efficacy data, and concerns about side effects.13 27 Nonetheless, in our study population, virtually no HCW was outrightly vaccine-averse, only unsure, suggesting that the underlying reasons for vaccine hesitancy may be modifiable factors that could be intervened on with tailored interventions to increase vaccine coverage, including boosters. COVID-19 booster vaccines can strengthen waning immunity, widen the range of immunity against new variants and increase protection for HCWs.28
Addressing vaccine hesitancy among pharmacy staff is particularly important given the fact that pharmacies are a key location for vaccine administration. Vaccine hesitancy among personnel in pharmacies could potentially hamper effective communication to clients about the importance of getting vaccinated.
Contrary to expectations early in the pandemic that African American communities would be the most resistant towards COVID-19 vaccines,29 30 non-Hispanic blacks in our sample reported very high vaccination rates and did not differ significantly from non-Hispanic whites within adjusted analysis. In a longitudinal study with monthly follow-up conducted during December 2020 to June 2021, vaccine hesitancy decreased more rapidly among black individuals than among White individuals.31 Similarly, a US national study examining COVID-19 vaccination coverage by race and ethnicity during December 2020–November 2021, found that whereas Hispanic (47.3%), non-Hispanic black (46.3%) adults had lower ≥1 dose coverage by the end of April 2021 when compared with non-Hispanic white adults (59.0%), these differences had disappeared by the end of November 2021.32 These trends appear to be driven by the observation that Black individuals more rapidly came to believe that vaccines were necessary to protect their communities.31 Taken together, achieving progress in reducing disparities in vaccine uptake therefore requires a nuanced understanding of risk/protective factors and how underlying patterns and reasons for vaccine hesitancy may have changed over time. Understanding the intertwined effects of various individual, interpersonal and environment risk/protective factors on vaccine hesitancy can better inform targeted, equity-based interventions. Ensuring the population stays informed and aware about safety and any concerns related to adverse events regarding approved vaccines may foster transparency and improve trust in the vaccines.
Black and Hispanic HCWs were more likely to be ever diagnosed of COVID-19 than their white counterparts even after adjusting for vaccination status and several sociodemographic characteristics. HCWs of colour are more likely to serve in communities of colour which typically have smaller facilities, fewer resources (including personnel), and higher patient load, all of which may increase risk of exposure and infection to HCWs in these settings.25 26 33–35 To achieve a positive equity impact, it will be important to address these constraints so that communities of colour are better empowered to respond to current and future public health threats. Within the context of the current pandemic, there is also need for comprehensive implementation of both ‘backward tracing’ (identifying sources of infection), as well as ‘forward tracing’ (identifying contacts) as part of concerted efforts to break chains of COVID-19 transmission in healthcare settings and the broader community.
The findings in this report are subject to several limitations. First, self-reported measures may be subject to misreporting, including employment setting, COVID-19 diagnosis and vaccination status. Within the pooled sample, close to 5% (n=21, 568) did not provide information on their work setting, and this may have included some HCWs. There may be selection bias if there were systematic differences between HCWs who responded vs those who did not respond. Second, small sample sizes for some population subgroups resulted in some imprecise estimates. Third, we did not assess exposure source for those with self-reported ever COVID-19 diagnosis; we are, therefore, not able to differentiate between HCWs that were exposed in the community vs exposed at work. Finally, we urge cautious interpretation of our measures of association as they do not imply causation.
Conclusion
Of HCWs surveyed in the New York Metropolitan area during the study period, 92.3% reported being fully vaccinated, and 20.9% had ever been diagnosed of COVID-19. Pooled analysis of nationwide data revealed that the odds of ever COVID-19 diagnosis among HCWs varied by vaccination status, sociodemographic characteristics, and type of healthcare facility. Some options to achieve a positive equity impact in COVID-19 vaccine uptake among HCWs could include improving vaccine accessibility, providing incentives, as well as implementing mandates. As the need for booster doses becomes readily apparent in the rapidly evolving COVID-19 landscape, there is need for more engagement around vaccine hesitancy to better understand risk/protective factors and how reasons for vaccine hesitancy may have changed over time. Maintaining high vaccination coverage among HCWs is particularly important to reduce opportunities for transmission within facilities, especially in settings where the risk of exposure is high.
Data availability statement
Data are available in a public, open access repository. US Census Bureau. Measuring Social and Economic Impacts during the Coronavirus Pandemic. Available at https://www.census.gov/programs-surveys/household-pulse-survey.html. Accessed on 31 December 2021.
Ethics statements
Patient consent for publication
Ethics approval
These analyses involved use of unidentifiable publicly available data, and thus qualifies as nonhuman research under the Common Rule (45 CRF 46); therefore, ethical review was not sought.
References
Footnotes
Contributors IA conceptualised and designed the study and drafted the initial manuscript. AD, AF, AB, SA, MM and TL helped conceptualise the study and critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work. IA had full access to all of the data in the study and takes responsibility for the intergrity of the data and the accuracy of the data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.