Article Text

Abstract
To describe the methodology of development of a protocol for application of the Brazilian Dietary Guidelines by primary healthcare professionals in individual dietary advice. A five-step approach was followed: (1) format definition; (2) definition of the instrument for assessment of individuals’ food consumption; (3) Dietary Guidelines’ content extraction; (4) protocol content development; (5) content and face validity. An example from Brazil was displayed with the development of a protocol to guide healthcare professional decision-making when providing nutrition advice based on the Brazilian Dietary Guidelines. The instrument of the Brazilian Nutrition Surveillance System (SISVAN) was chosen to the food consumption assessment, which contains questions about the consumption of seven healthy or unhealthy food groups and one question about eating modes. The Guidelines’ content extraction process led to the identification of recommendations related to the food consumption markers assessed by the SISVAN questionnaire. Then, a protocol was developed in a flowchart format, in which the professional’s conduct is guided by the answer given to each question of the SISVAN instrument. For each ‘non-compliant’ answer (unhealthy eating practice), the professional is instructed how to provide recommendations and identify obstacles. Lastly, experts and healthcare professionals highlighted pertinence, clarity and usability of the protocol. This study provides the blueprint for the phase-wise development of protocols of application of the Dietary Guidelines and may contribute to promote healthier eating and ending malnutrition in all its forms.
- primary health care
- practice guidelines as topic
- diet
- healthy
- health promotion
- health services
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Malnutrition in all its forms, including underweight, micronutrient deficiencies, overweight and unhealthy eating, is the leading cause of disease worldwide. In recent years, the health effects of global warming have begun to considerably exacerbate these problems.1–3 These epidemics affect people of all life cycles in most countries of the world and represent what is now called the Global Syndemia, as they interact with each other in time and space and in their consequences, in addition to sharing common causes, including the characteristics of the globalised food system.4
Within this context, international organisations recognise National Dietary Guidelines as a ‘multiple-duty’ action to support the reorientation of food systems and mitigate the Global Syndemic. Dietary Guidelines detail the most recent scientific evidence regarding the relationship between diet and health and provide advice on healthy food choices to reduce obesity and undernutrition, and can ideally be extended to include recommendations on environmentally sustainable diets.4 5 They serve as the foundation for actions on nutrition education, and are the basis of national policies on food security and school meals.6 In Brazil, the most recent edition of the Dietary Guidelines was published in 2014 by the Ministry of Health, presenting evidence-based recommendations for the population referenced on a new paradigm that takes into account the importance of food processing, meal structures and modes of eating, as well as the relationship between diet and the environment.7
In 2020, the Global Nutrition Report called attention to the importance of integrating nutrition actions into health systems and highlighted primary healthcare as a priority locus for these actions.8 As the most inclusive, equitable, cost-effective and efficient whole-of-society approach, primary healthcare services have a huge potential to promote healthier eating and contribute to prevent and treat undernutrition and diet-related chronic diseases, benefiting particularly those less privileged and of lower socioeconomic status.8
Despite this, the promotion of healthy eating is frequently underprioritised to the detriment of medical, drug treatment-based care and it is still insufficiently integrated into primary healthcare. A previous study showed that about two-thirds of the primary care practitioners provided dietary counselling for 40% or less of their patients and spent 5 min or less discussing dietary pattern changes.9 Recently, a study described that only 12% of the medical appointments included counselling about diet, even among high-risk patients with non-communicable diseases.10 Among the main barriers identified to the incorporation of nutrition actions, we highlight lack of time, inadequate knowledge on nutrition, low self-efficacy for counselling patients about diet, insufficient professional qualification and absence of practical supporting materials.9–15
In this sense, it is recognised that the creation of clinical guidelines can be an effective action to increase the implementation of Dietary Guidelines and to reduce inappropriate practice and improve the quality and efficiency of nutrition care. Guidelines from the WHO states that they should be developed with a systematic approach, evidence-based and with planned dissemination, implementation and evaluation strategies.16 Although different methodologies can be applied to build a clinical protocol, few studies have documented this process. Thus, this study aims to describe the development of a protocol for application of the Brazilian Dietary Guidelines by primary healthcare professionals in individual dietary advice.
Methodological design
This present study seeks to further the evidence in implementation science by presenting methods undertaken in the development of a clinical protocol to support the primary healthcare professionals in individual dietary advice.
The protocol needs to be developed by a steering committee composed by selected researchers free of conflicts of interest and with broad expertise on recommendations for healthy eating, dietary advice and primary healthcare system, which take responsibility on overall leadership by the protocol development. The protocol should be based on official recommendations for healthy eating, which are preferably established by the current national Dietary Guidelines.
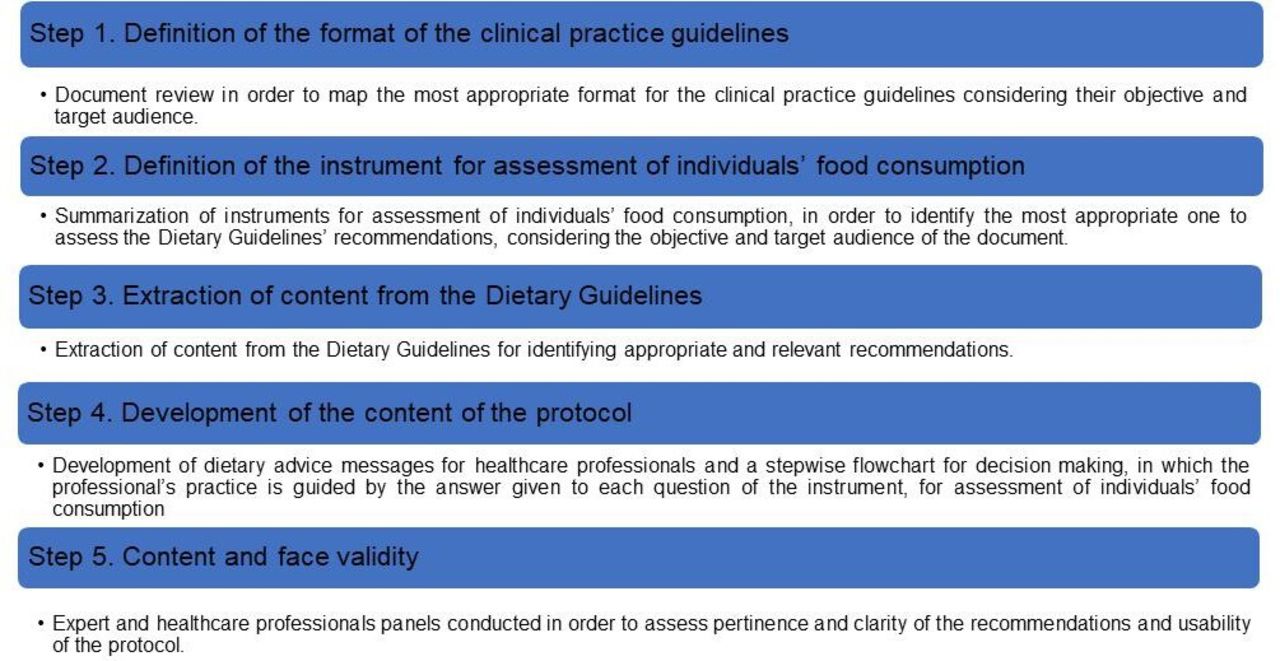
A five-step approach can be followed for developing the document (see figure 1): (1) definition of the format of the clinical practice guidelines (ie, in what structure and in what type of document the guidelines will be made available); (2) definition of the instrument for assessment of individuals’ food consumption; (3) extraction of content from the Dietary Guidelines; (4) protocol content development; and (5) content and face validity.

Sequential approach used for developing clinical practice guidelines for application of the Brazilian Dietary Guidelines by primary healthcare professionals in individual dietary advice. Brazil, 2020.
Step 1: format definition
Clinical practice guidelines are statements systematically developed to assist health professionals in deciding about appropriate healthcare for specific clinical circumstances. They are tools to help decision-makers make better decisions based on the best available evidence.17 18 The format varies according to their objective, the target audience and the characteristics of the healthcare service. They can be focused, for example, on the diagnosis, treatment or care of diseases or specific clinical conditions (at primary healthcare or at the hospital environment), in education or health promotion or even in the application of technologies or in the organisation of health services.
Researchers from the steering committee may carry out a review of international documents with orientations for the preparation of clinical practice guidelines (such as those from the WHO and the Institute of Medicine), as well as guidelines for primary healthcare already in use in the country (usually available at the website from the Ministry of Health). The review can be done through searches in scientific databases such as PubMed and Web of Science (using keywords such as ‘clinical protocols’ and ‘primary healthcare’), but also on websites of organisations such as the WHO and the national Ministry of Health. The goal is to map possible formats, systematically analyse their characteristics and identify the most applicable one to guide dietary advice during individual appointments in primary healthcare. Based on this, the steering committee will define the scope, format and broad sections of the clinical practice guidelines.
Step 2: definition of the instrument for assessment of individuals’ food consumption
The decision-making regarding the dietary advice messages is based on the assessment of individuals’ food consumption. Because of this, the steering committee reviews all existing instruments for assessing food consumption in the country. The review can be done through searches in scientific databases such as PubMed and Web of Science (using keywords such as ‘questionnaire’ and ‘food consumption’), but also in grey literature (national surveillance systems or theses/dissertations). The objective is to identify a short instrument to assess the main recommendations for healthy eating that could be used by any primary healthcare professional (regardless of their specialty) during the appointments.
Step 3: the Dietary Guidelines’ content extraction
Is this step, members from the steering committee (ideally two) independently carry out a systematic reading of the Dietary Guidelines in order to identify appropriate and relevant recommendations that are in line with the indicators of the instrument for assessment of individuals’ food consumption (ie, recommendations on the consumption of foods/food groups that are assessed in the instrument defined in Step 2).
Moreover, they also identify additional recommendations that are considered relevant to be included in the document, even if they were not addressed by the instrument for assessment of individuals’ food consumption. A broader group of researchers from the steering committee check for consistency and then analyses the recommendations to set down the final list.
Step 4: protocol content development
In this step, the steering committee carries out the development of the messages of dietary advice for the health professionals and the diagramming of the document based on Steps 1–3.
The recommendations extracted from the Dietary Guidelines in the Step 3 may be converted into messages of dietary advice for healthcare professionals. That is, unlike the Dietary Guidelines themselves, that state the recommendations for healthy eating (for example: Healthy dietary patterns include a variety of vegetables), in the protocol the messages are directed to healthcare professionals and written in order to facilitate their conduct during the individual appointment (for example: Recommend that individuals increase their consumption of vegetables).
Next, a stepwise flowchart for decision-making is developed, in which the answer given to each question of the instrument for assessment of individuals’ food consumption guides the health professionals towards the messages of dietary advice. See below an example:
Question of the instrument for assessment of individuals’ food consumption: Do you usually eat fruits?
Recommendation of the national Dietary Guidelines of the country on this food group: Healthy dietary patterns include a variety of fruits.
Individual’s answers (possibilities): Yes/No.
Instructions for the healthcare professionals in the clinical protocol:
In case the individual has answered ‘no’ to the question, advise on the importance of increasing fruit consumption. Explain the justification for this recommendation and investigate the reasons why this food is not present in the individual’s diet.
In case the individual has answered ‘yes’ to the question, encourage the individual to continue this practice.
The flowchart may have one or more starting and ending points. They can be orientated vertically or horizontally. The geometric figures on the flowchart represent the steps of the process and are connected with arrows that show the sequence of the actions. Special shapes represent different types of actions and process steps. The document should be written in the local language (or languages), including instructions to the professionals on how the protocol should be used, the instrument for assessment of individuals’ food consumption, the stepwise flowchart and the instructions for the health professionals on how to deliver the dietary advice messages.
Step 5: content and face validity
Finally, the protocol should be submitted to content and face validity19–22 through panels with experts and primary healthcare professionals, and both of them recorded. Experts with background on the Dietary Guidelines and/or background on clinical protocols attend the content validation process. They evaluate the clarity and relevance of the recommendations and images, and provided suggestions for the document. Primary healthcare professionals who have university degrees in health sciences and worked in the different regions of the country attend the face validity process. The face validity aims to identify the usability, the understanding of the content and the applicability of the protocol by its ‘end users’.
The data obtained from experts and professionals’ panels can be analysed using thematic content analysis.23 The operationalisation steps are: (1) preanalysis: transcription of the recordings and definition of possible themes to guide the analysis; (2) exploratory reading of the transcripts: identification of the emerging themes and categories with double analysis and checking by a third researcher and elaboration of the codebook with description of the characteristics, criteria of inclusion and exclusion and examples of each category; (3) analysis of the results: codification of the excerpts of the transcripts and elaboration of the summarisation of the results; (4) inference and interpretation: based on the results, the steering committee carry out the relevant and appropriate modifications in the protocol.
The example from Brazil
This section presents the methods undertaken in the development of a protocol to support the application of the Brazilian Dietary Guidelines by primary healthcare professionals in individual dietary advice. The proposed protocol was developed by a steering committee composed by seven researchers free of conflicts of interest and with broad expertise on the Dietary Guidelines for the Brazilian Population, dietary advice and the Brazilian primary healthcare system.
The Dietary Guidelines for the Brazilian Population
The Dietary Guidelines for the Brazilian Population, published by the Brazilian Ministry of Health in 20147 is an official document that presents evidence-based recommendations for healthy eating for the Brazilian population. They are part of Brazil’s concerted effort in promotion of health and prevention of diet-related diseases. They are systematised into a document with five chapters. The first chapter presents the principles that guide its elaboration. Chapter 2 presents recommendations for food choices based on the Nova (a name, not an acronym) classification system, which categorises food based on the characteristics of industrial processing. The golden rule is ‘always prefer natural or minimally processed foods and freshly made dishes and meals to ultra-processed food’. Chapter 3 discusses how to combine foods into meals and provides recommendations on variety and forms of preparing many natural or minimally processed foods that are usually part of the traditional Brazilian diet. Chapter 4 discusses modes of eating and the way time and attention devoted to eating, the environment where it takes place and the sharing of meals influence the quality of the diet and the pleasure to eat. Lastly, Chapter 5 exposes possible obstacles to adhering to the recommendations—such as information, supply, cost, cooking skills, time and advertising—and suggests ways to overcome them.
The Brazilian Dietary Guidelines’ recommendations are summarised in 10 steps:
Make natural or minimally processed foods the basis of your diet;
Use oils, fats, salt and sugar in small amounts when seasoning and cooking natural or minimally processed foods and to create culinary preparations;
Limit consumption of processed foods;
Avoid consumption of ultra-processed foods;
Eat regularly and carefully in appropriate environments and, whenever possible, in company;
Shop in places that offer a variety of natural or minimally processed foods;
Develop, exercise and share cooking skills;
Plan your time to make food and eating important in your life;
Out of home, prefer places that serve freshly made meals;
Be wary of food advertising and marketing.
Step 1: format definition
The clinical practice guidelines were organised in a format of a short ‘standardised protocol for use’ (in Portuguese, Protocolo de Uso), which sets a sequence of steps to guide professional decision-making in using a technology (ie, the Dietary Guidelines), defined by the WHO as the ‘application of organised knowledge and skills in the form of instruments, devices, medicines, vaccines, procedures, and systems developed to solve a health problem and improve quality of lives’.24 Its central element is a decision flowchart guided by the prior assessment of individuals’ food consumption. The protocol was designed to be used by any primary healthcare professional who has a university degree, regardless of specialty, during individual appointments.
Step 2: definition of the instrument for assessment of individuals’ food consumption
The instrument of the Brazilian Nutrition Surveillance System (SISVAN) was chosen for the assessment of individuals’ food consumption (hereafter called ‘SISVAN instrument’). This instrument assesses the adherence to the main recommendations of the Dietary Guidelines for the Brazilian Population. In addition, it is short, applicable during individual appointments and officially integrates the National Health Information System. As such, it is already part of the in-service surveillance actions performed by all primary healthcare professionals (regardless specialty) and eliminates the need for specific training for its use within the protocol.
The SISVAN instrument is a short questionnaire for individuals aged 2 years or above containing questions (yes/no) about the consumption in the previous day of four categories of ultra-processed foods (hamburger, and/or other reconstituted meat products; sugar-sweetened beverages; instant noodles, salty snacks and/or crackers; cookies, candies and/or other confectionery, that are indicators of unhealthy eating), three categories of natural or minimally processed foods (beans, fruits and vegetables, that are indicators of healthy eating) and one question about eating modes (habit of eating while watching television or using the computer/mobile) (see figure 2).

SISVAN (Brazilian Nutrition Surveillance System) instrument for assessment of individuals’ food consumption. Brazil, 2020. *Self-translation by the authors of the study.
Step 3: the Brazilian Dietary Guidelines’ content extraction
Two researchers (CRT and JGLdJ) carried out a systematic reading of the Chapters 2 (choosing foods), 3 (from foods to meals), 4 (modes of eating) and 5 (understanding and overcoming obstacles) of the Dietary Guidelines for the Brazilian Population in order to identify appropriate and relevant recommendations that were in line with the indicators of the instrument for assessment of individuals’ food consumption (ie, recommendations on the consumption of foods/food groups that are assessed in the instrument defined in Step 2).
Moreover, the same researchers (CRT and JGLdJ) also identified additional recommendations that were considered relevant to be included in the document, even if they were not addressed by the instrument for assessment of individuals’ food consumption. These recommendations were added because they are addressed in the Dietary Guidelines for the Brazilian Population and considered important by the researchers of this project. Most of these recommendations do not necessarily refer to specific foods/food groups, but ways of eating and how to overcome obstacles to healthy eating. The other five members of the steering committee checked for consistency and reviewed the recommendations to set down the final list.
The Brazilian Dietary Guidelines’ content extraction process led to the identification of a list of 99 recommendations related to the food consumption indicators assessed by the SISVAN instrument.
For healthy eating indicators, recommendations include general guidance on their consumption, suggestions on variations and ways of preparing these foods, a summary of the evidence that justify why these recommendations are important to follow and possible obstacles and strategies to overcome them. For unhealthy eating indicators, the recommendations include general guidance on their consumption, suggestions of healthy alternatives to replace these foods, a summarisation of the evidence that justify why these recommendations are important to follow and possible obstacles and strategies to overcome them. For the question about eating while watching television or using the computer/mobile, the recommendations include a general orientation on this practice, suggestions on how to change this habit and summarisation of the evidence that justify why these recommendations are important to follow.
Furthermore, five additional recommendations from the Dietary Guidelines were identified, which, although not directly related to the food consumption indicators assessed by the SISVAN instrument, were considered relevant to be included in the protocol. These include, for example, warnings on the effects of food advertising, information about organic foods and recommendations for people with financial constraints.
Step 4: protocol content development
The recommendations extracted from the Dietary Guidelines for the Brazilian Population in the Step 3 were converted into messages of dietary advice for healthcare professionals.
The document was written in Portuguese and its content was divided into six subsections:
Introduction (with brief information on the Dietary Guidelines for the Brazilian Population, the purpose of the protocol and general instructions on the approach in carrying out dietary advice).
Sequential instructions on how the protocol should be used (for example: complete the instrument for assessment of individuals’ food consumption, follow the stepwise flowchart and provide dietary advice).
Instrument for assessment of individuals’ food consumption.
Stepwise flowchart.
Dietary advice messages related to the food indicators of the SISVAN instrument for the health professionals.
Additional messages.
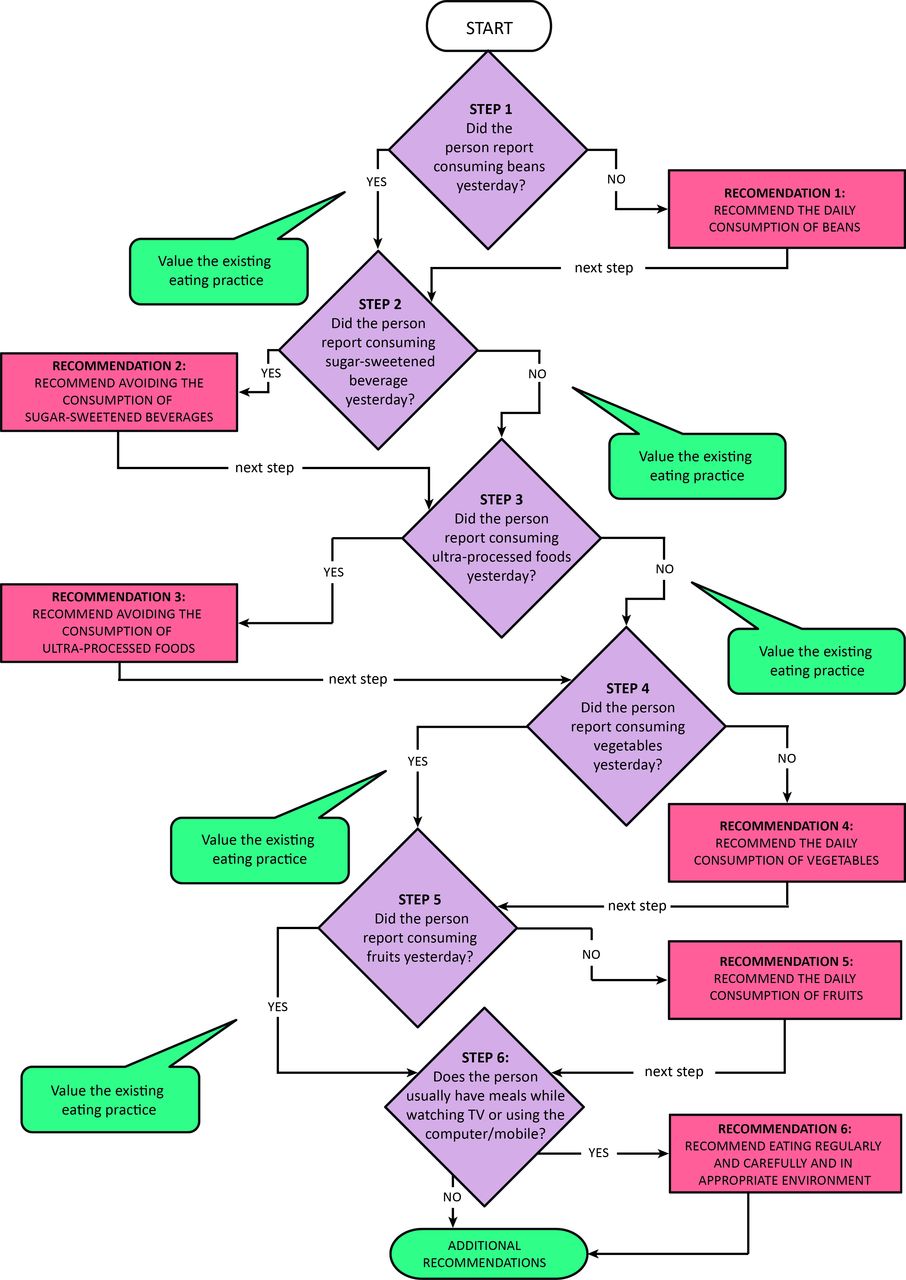
Figure 3 presents the stepwise flowchart for decision-making. Different geometric figures represent different steps in the decision-making process. The diamonds contain the questions of the SISVAN instrument (p.e. ‘Did the persons reported consuming beans?’) and the rectangles the dietary advice messages (p.e. ‘Recommend the daily consumption of beans’).
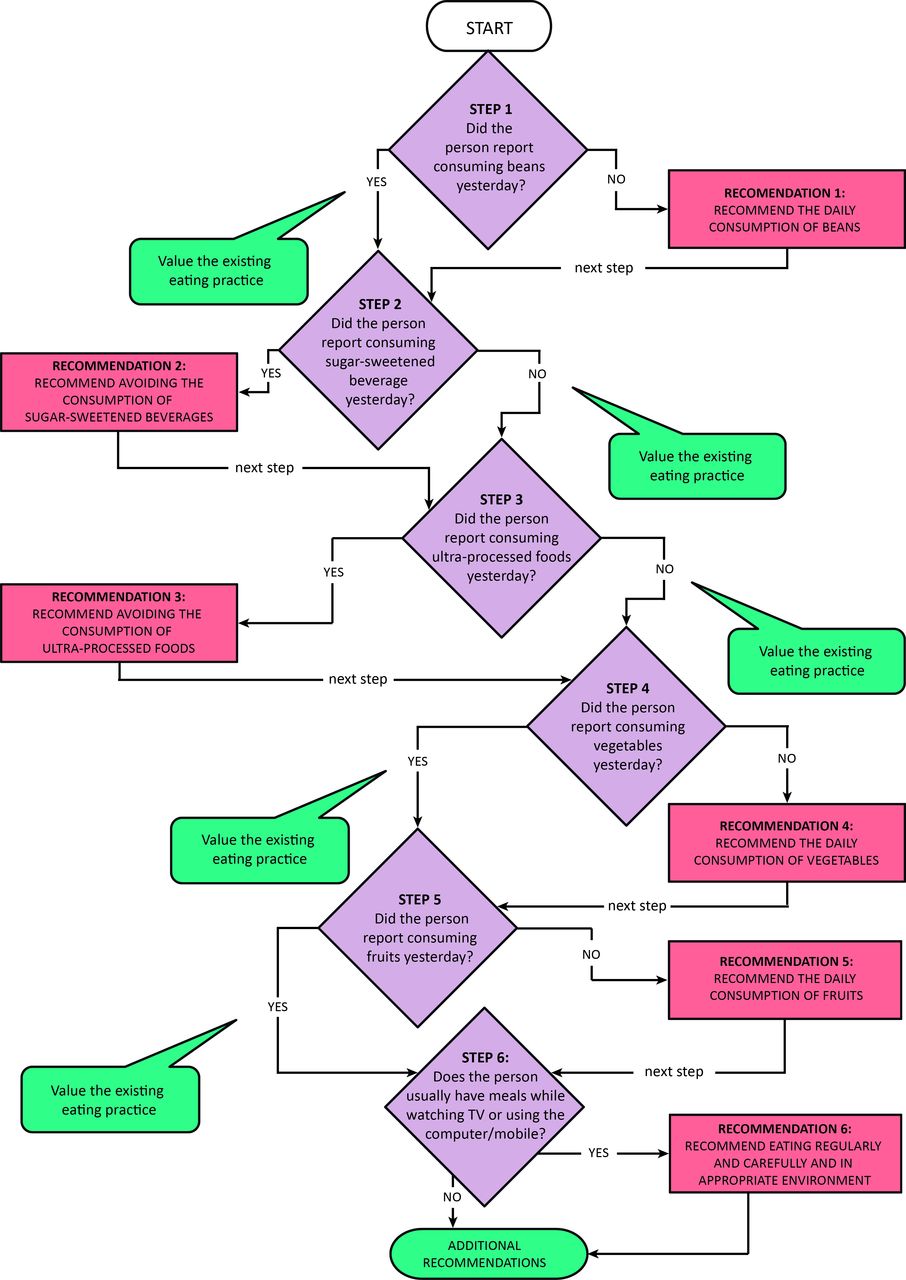
Stepwise flowchart for decision-making. Brazil, 2020. *Self-translation into English by the authors of the study.
The steps in the flowchart aim to progressively address the recommendations of the Dietary Guidelines for the Brazilian Population, starting from their golden rule ‘always prefer natural or minimally processed foods and freshly made dishes and meals to ultra-processed foods’. The evaluation of the golden rule is indirectly made through the question on the consumption of beans—the basis of one of the most important Brazilian culinary preparations and a strong indicator of the consumption of freshly prepared meals—and by the questions on the consumption of ultra-processed foods, represented by sugar-sweetened beverages, hamburger and/or other reconstituted meat products, instant noodles, salty snacks and/or crackers and cookies, candies and/or other confectionery. Then, the flowchart addresses the consumption of fruits and vegetables, which daily consumption is a complementary recommendation of the Dietary Guidelines for the Brazilian Population. Finally, the flowchart addresses the habit of eating meals while watching television or using the computer/cell phone, understanding it as an indicator of inappropriate modes of eating.
Based on individuals’ answers to the SISVAN instrument, the health professional must follow the flowchart and provide dietary advice (see table 1, for examples). For each ‘non-compliant’ answer (unhealthy eating practice), the professional is instructed how to provide recommendations and identify possible obstacles to their adherence. For each ‘compliant’ answer (healthy eating practice), the healthcare professional is instructed to value the existing eating practice. There are no guidelines on how many recommendations should be provided per appointment since it depends a lot on the consultation time (and this varies according to each service) and other demands from the individuals. The healthcare professional can decide to make priority recommendations in the first appointment and follow with the other advices in the next appointments.
Examples of messages of dietary advice for healthcare professionals. Brazil, 2020
Step 5: content and face validity
The protocol was submitted to content and face validity19–22 through seven online panels with experts and primary healthcare professionals, and all of them were recorded. In content validity, experts provided online consent. In face validity, primary healthcare professionals provided a written consent. Experts with background on the Brazilian Dietary Guidelines and/or background on clinical protocols attended the content validation process. The panels aimed to discuss the relevance, clarity, usability, understandability and applicability of the protocol with the participants and collected suggestions for the document. The leading questions of the content validity panel were ‘What were the general impressions of the protocol? How clear and pertinent is the protocol to use for professionals around the country?’ Primary healthcare professionals who had university degrees in health sciences and worked in the five major regions of Brazil attended the face validity process. The face validity aimed to identify the usability, the understanding of the content and the applicability of the protocol by its ‘end users’. The leading questions of the face validity panel were ‘How clear is the use of the protocol? How clear is the content? How usable is the protocol?’ Thirty-three experts attended the content validity (out of 35 that were invited) and 14 professionals the face validity (out of 25 that were invited).
CRT, JGLdJ and TSSS evaluated the data obtained from experts and professionals’ panels using thematic content analysis.23 The operationalisation steps were: (1) preanalysis: transcription of the recordings and definition of possible themes was done to guide subsequent analysis; (2) exploratory reading of the transcripts: this was done to identify emerging themes and categories by two researchers (CRT and JGLdJ). A third researcher checked all theme categorisation (TSSS). This resulted in the elaboration of the codebook that contained a description of the themes, criteria for their identification and examples; (3) analysis of the results: excerpts of the transcripts were coded, and all results were summarised; (4) inference and interpretation: based on the results of the coding process the steering committee suggested modifications to the protocol that were then incorporated.
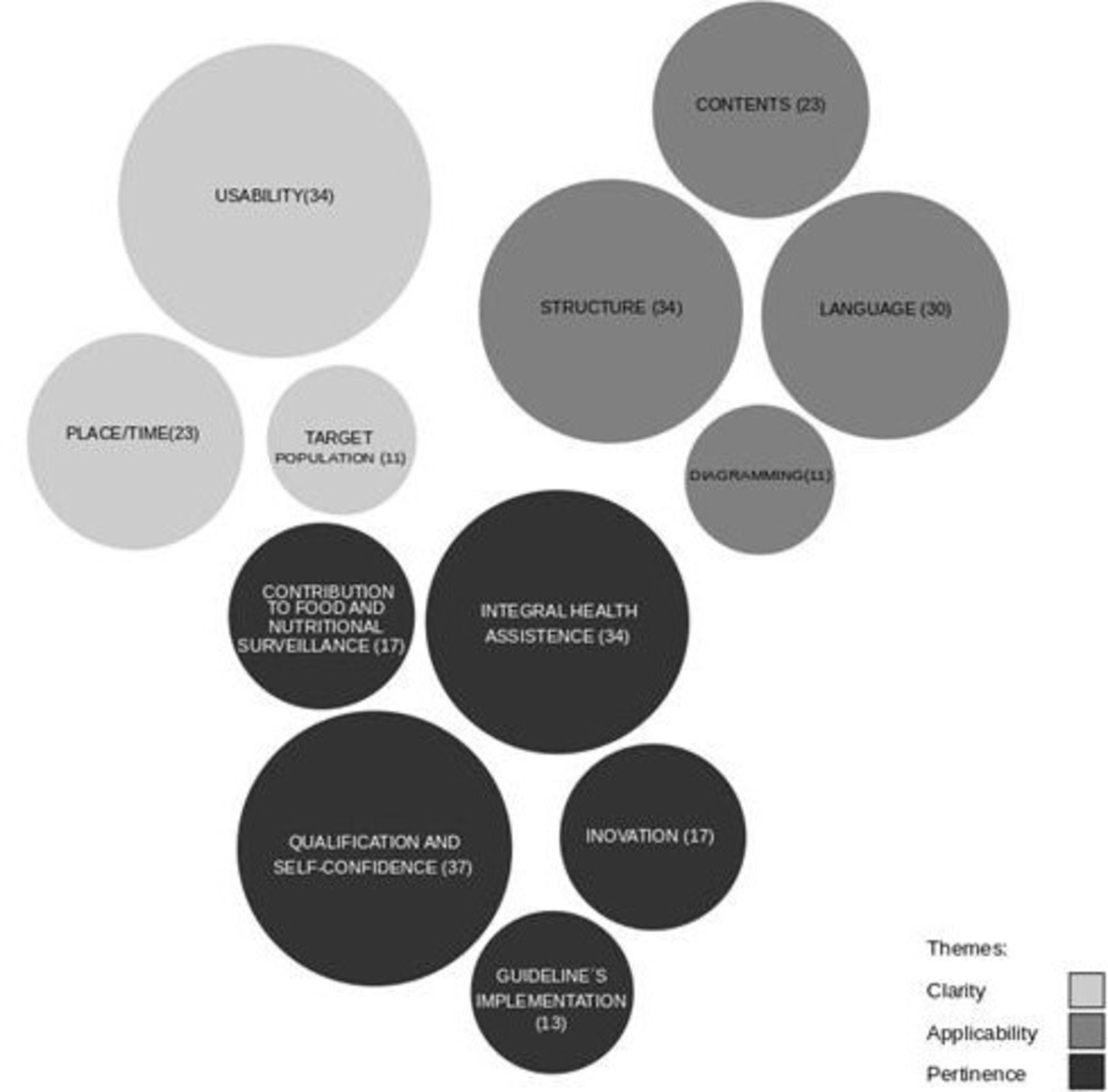
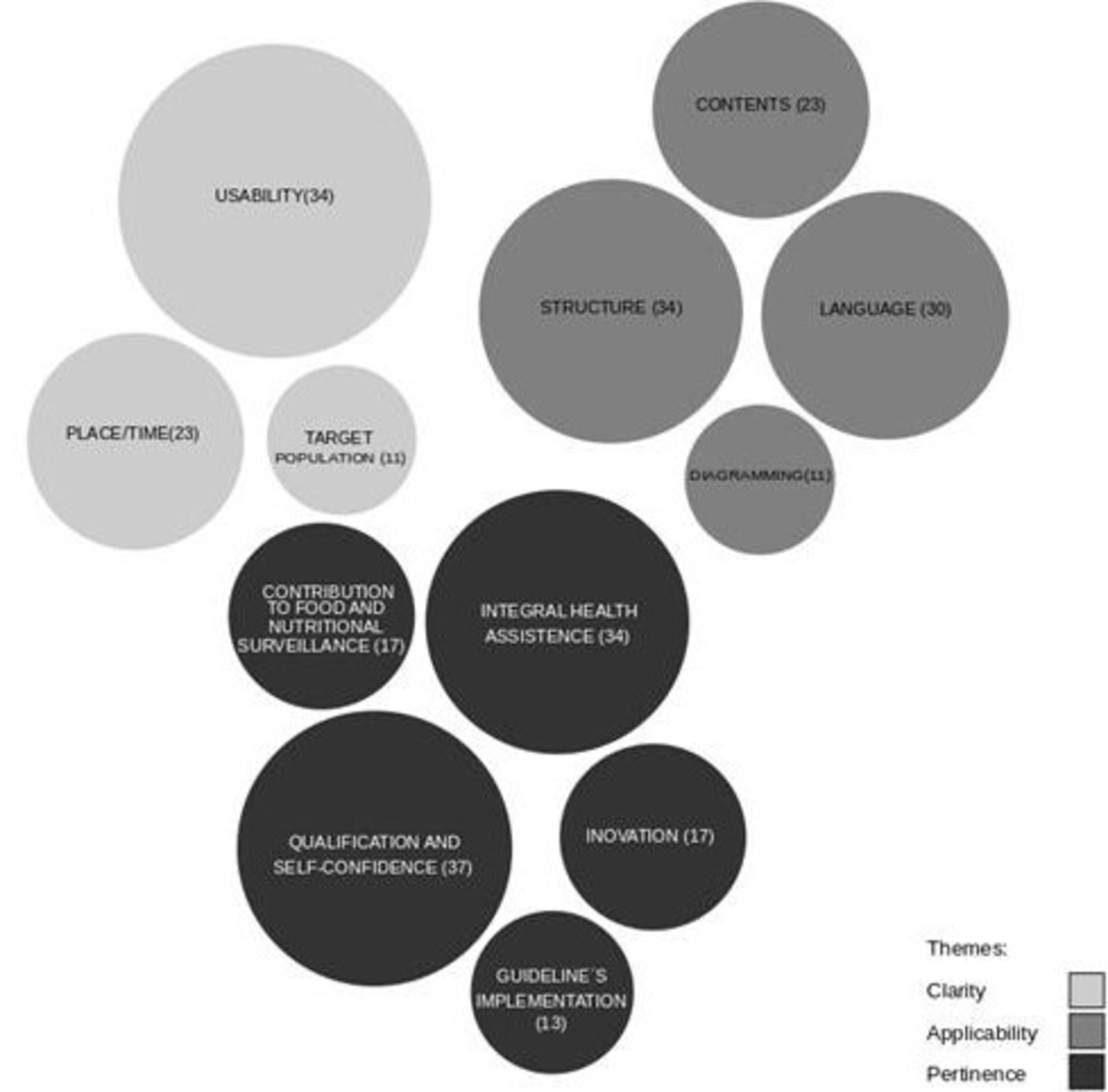
The transcripts of seven panels were analysed (four from experts and three from professionals). The themes identified were pertinence (with five subcategories of analysis), clarity (with three subcategories of analysis) and applicability (with four subcategories of analysis). Figure 4 shows the identified themes and subcategories. The size of each circle is directly related to the number of times that each subcategory appeared in the analysis, meaning that the larger the circle, the more often the subcategory was present in the statements. In the pertinence theme, excerpts highlighted the contribution (or not) of the protocols for: implementation of the Brazilian Dietary Guidelines; integral healthcare, food and nutritional surveillance and the use of the SISVAN instrument, professionals’ qualification and confidence for dietary advice and innovation in individual dietary advice in the primary healthcare setting. When assessing the protocol’s clarity, that is, if the protocol content was (or was not) clear and understandable, excerpts about the protocol structure (format, components of the protocol and flowchart), the language and technical terms, diagramming and understanding of technical content stood out. Regarding the applicability, that is, possibilities, facilities or limits for the use of the protocol in primary healthcare, there were highlighted excerpts about the usability of the protocol in different regions and realities of the country, the application of the protocol by different health professionals (regardless specialty), the use of the protocol as a supportive tool for these professionals, the contexts where the protocol could be used and the time spent for its use.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Emerging themes, frequency and categories of the thematic analysis of the panels with expert and health professionals. Brazil, 2020.
The published version of the protocol can be found at The Brazilian Ministry of Health website (in Portuguese): https://bvsms.saude.gov.br/bvs/publicacoes/protocolos_guia_alimentar_fasciculo1.pdf (access in 6 out 2021).
Discussion
This study provides the blueprint for the phase-wise development of a clinical practice guideline to support primary healthcare professionals in individual dietary advice and describes an example using the Brazilian Dietary Guidelines. The multistep methodology includes the selection of a practical method for assessing individuals’ food consumption, the extraction of the Dietary Guidelines’ recommendations and subsequent development of a protocol with messages of dietary advice and a stepwise flowchart for decision-making. Additionally, the pertinence, clarity and usability of the protocol are evaluated in panels with experts and healthcare professionals. The result is a short, practical and easily applicable standardised protocol that encompasses the main recommendations from the national Dietary Guidelines.
To the best of our knowledge, this is the first study that proposes the development of a clinical practice guideline for healthy eating promotion in primary healthcare services. In 2013, the American Association of Clinical Endocrinologists published a clinical practice guideline for healthy eating for the prevention and treatment of metabolic and endocrine diseases in adults. Although the document targets health professionals in general, its main recommendations involve the prescription of diet plans based on nutrient adequacy and calorie control, an approach that requires specific professional qualification, which may make its application in primary healthcare services difficult.25 More recently, Obesity Canada and the Canadian Association of Bariatric Physicians and Surgeons published a clinical practice guideline for obesity care by primary healthcare professionals. Although the document recognises that dietary advice is a foundation for obesity management, it does not provide specific guidance on how to promote healthy dietary patterns.26 The methodology used in our study may be easily adapted to different countries, while taking into consideration their own National Dietary Guidelines, the available resources and local characteristics. This protocol was design for a context of primary healthcare appointments and, therefore, is not intended to cover all nutritional care needs. Many people, therefore, with more specific nutritional needs, may need more complete and specialised approaches.
In Brazil, the Unified Health System (named SUS) must guarantee universal, equitable and integral access to actions on health promotion, including those related to nutrition.27 Among the actions from SUS concerning nutrition, those aiming at promoting healthy eating are especially relevant, which include initiatives focused on health public policies, the creation of healthy environments, the development of personal skills and the reorientation of health services.28 Primary healthcare is the entry point to the system and is responsible for offering multiprofessional and lifelong care to individuals, families and communities who live in a given territory.29
Despite the strengthening of these actions over the years, however, there are still challenges for the qualification of nutritional care in primary healthcare in Brazil.15 30 If, on the one hand, there is difficulty for healthcare professionals to carry out actions on healthy eating promotion, whether due to lack of qualification and training or constraints in the daily routine; on the other hand, the content of dietary recommendations—materialised in the form of traditional, prescriptive, nutrient-centred food guides—makes this approach even more difficult to be implemented by multiprofessional teams. These difficulties, however, are not unique to Brazil. In Australia, general practitioners and nurses had limited faith in their knowledge and experience to provide nutrition counselling effectively, and agreed they required more nutrition information to effectively provide nutrition advice.31 In Canada, a study identified an important gap between the number of patients who respondents that would benefit from nutrition counselling and the proportion who received such counselling, and almost all physicians identified lack of time and compensation as the strongest barriers to providing nutrition guidance.12
Despite that, the Brazilian Dietary Guidelines seek to overcome these limitations by providing technical information with important conceptual innovations and a paradigm that is in line with the knowledge and competences of all healthcare professionals (not only dietitians or nutritionists). First, the Brazilian Dietary Guidelines consider that food is more than nutrient intake and account for the social, cultural, economic and environmental implications of eating. Additionally, their main recommendations are based on a classification system that categorises foods based on the characteristics of the industrial processing instead of their nutritional profile. The approach is qualitative and the guidelines do not provide advice on amounts of calories or nutrient requirements. There is also a realistic and doable perspective. Most of the recommendations were based on the analysis of a nationally representative intake survey, which evaluated data on food consumption by more than 30 000 Brazilians from all the regions of the country. Lastly, the guidelines recognise that the recommendations are not always easy to be followed and present strategies for overcoming barriers to healthy eating.32 Although freely available online, and disseminated through social media websites, however, it is unlikely that the Dietary Guidelines—with a large number of recommendations described in 158 pages—will be easily incorporated into the routine of the primary healthcare services without a practical instrument that supports their professionals.
While the importance of best practices for creating clinical guidelines has been extensively emphasised,16–18 few studies have documented their process of development. The clinical protocol presented in this study was based on rigorous and reproducible methods, and validated with the participation of end users. The content and face validity processes used in the development of the Brazilian protocol, however, may have some limitations. The difficulties imposed by the online panel and the unavailability of the health professionals’ agenda to participate in the panels and read the protocol (worsened by the COVID-19 pandemic) may have reduced the engagement in the discussions. In order to get around this, however, the panels were scheduled after work period, the meetings were shorter and the professionals could indicate their colleagues to replace them in case they could not attend it.
Lastly, it is important to highlight that the success of the clinical protocol depends on effective strategies of implementation, which include dissemination among the target group, adoption by this group, implementation in actual practice and its maintenance in the daily routine.16 33 These actions will require targeted policy action, as well as advocacy efforts and engagement from healthcare providers. In January 2021, the protocol was published on the website of the Brazilian Ministry of Health,34 but other strategies still need to be executed in order to spread it throughout the country. The next phase of the study consists of adapting the protocol to different life cycles (pregnant people, elderly, children and adolescents). Methods and results from this step of the study will be reported in subsequent manuscripts. Future work will test the effectiveness of a training strategy for the use of the clinical protocol in improving the practice of healthcare professionals and the diet quality of individuals.
In conclusion, our study addresses the dearth of evidence on translating Dietary Guidelines into actionable and accessible protocols to guide professional practice in primary healthcare, furthering implementation science and potentially contributing to promote healthier eating and ending malnutrition in all its forms.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committe of the School of Public Health, University of Sao Paulo (4.232.862). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors MLdCL was responsible for planning and writing the draft of the manuscript. CRT, JGLdJ and TSSS evaluated the data obtained from experts and professionals panels and contributed in the writing of the paper. JRBH was the project manager and contributed in the writing of the paper. PCJ was responsible for planning and contributed in the writing of the paper and is the principal investigator of the project (the guarantor).
Funding The authors declare that this study received funding from Organização Pan-Americana da Saúde (OPAS - escritório Brasil)—Carta-Acordo SCON2019-00489. The study was granted ethical approval on 24 August 2020 by the Ethics Committee of the University of São Paulo (file number 4.232.862) and was conducted on behalf of the Brazilian Ministry of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.