Article Text

Abstract
Objective To evaluate the effect of a one-time cash transfer of $C1000 in people who are unable to physically distance due to insufficient income.
Design Open-label, multi-centre, randomised superiority trial.
Setting Seven primary care sites in Ontario, Canada; six urban sites associated with St. Michael’s Hospital in Toronto and one in Manitoulin Island.
Participants 392 individuals who reported trouble affording basic necessities due to disruptions related to COVID-19.
Intervention After random allocation, participants either received the cash transfer of $C1000 (n=196) or physical distancing guidelines alone (n=196).
Main outcome measures The primary outcome was the maximum number of symptoms consistent with COVID-19 over 14 days. Secondary outcomes were meeting clinical criteria for COVID-19, SARS-CoV-2 presence, number of close contacts, general health and ability to afford basic necessities.
Results The primary outcome of number of symptoms reported by participants did not differ between groups after 2 weeks (cash transfer, mean 1.6 vs 1.9, ratio of means 0.83; 95% CI 0.56 to 1.24). There were no statistically significant effects on secondary outcomes of the meeting COVID-19 clinical criteria (7.9% vs 12.8%; risk difference −0.05; 95% CI −0.11 to 0.01), SARS-CoV-2 presence (0.5% vs 0.6%; risk difference 0.00 95% CI −0.02 to 0.02), mean number of close contacts (3.5 vs 3.7; rate ratio 1.10; 95% CI 0.83 to 1.46), general health very good or excellent (60% vs 63%; risk difference −0.03 95% CI −0.14 to 0.08) and ability to make ends meet (52% vs 51%; risk difference 0.01 95% CI −0.10 to 0.12).
Conclusions A single cash transfer did not reduce the COVID-19 symptoms or improve the ability to afford necessities. Further studies are needed to determine whether some groups may benefit from financial supports and to determine if a higher level of support is beneficial.
Trial registration number NCT04359264.
- COVID-19
- preventive medicine
- health equity
Data availability statement
Data are available on reasonable request. The authors will disclose individual participant-level data on request after publication.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key points
Question
Physical distancing is a mainstay of controlling the COVID-19 pandemic but an insufficient income may make it difficult to remain at home, income increases could promote health during a pandemic by facilitating physical distancing.
Finding
A $C1000 cash transfer did not reduce exposure to COVID-19 based on symptoms or laboratory testing, but it did reduce COVID-19 symptoms in the prespecified subgroup of those older than 50 who were more likely to have symptoms.
Meaning
The findings suggest income supports targeted at those at higher risk of COVID-19 may be beneficial and that future evaluations could focus on older adults.
Introduction
Physical or social distancing, maintaining distance between individuals and avoiding gatherings by closing or reducing attendance at school and work, is effective at curbing the spread of epidemics based on systematic reviews of observational and modelling studies.1 Physical distancing during the COVID-19 pandemic was associated with reductions in COVID-19 spread between countries,2–4 but risk varies within countries based on individual characteristics such as racialisation and income.5–8
Income increases could promote health during a pandemic by facilitating physical distancing. In the USA, lower-income individuals were the most mobile group after state COVID-19 emergency declarations but the least mobile group prior based on mobile device location data.9 Modelling studies suggest that paid sick leave can reduce the spread of influenza-like illnesses by promoting adherence to physical distancing.10 11 Income supplements might also generally mitigate harms of pandemic related disruptions associated with unemployment or insufficient incomes. Multiple studies in a variety of settings have found that health is associated with income in general,12 and a pilot study of a basic income in Finland found improvements in reported health.13 Systematic reviews of cash transfers in low-income and middle-income countries indicate that they may improve some surrogate health outcomes.14 Many governments have made massive investments in cash transfers to individuals during the COVID-19 pandemic, but the effects of these income supports and the appropriate amount to provide are not known.
We conducted a randomised controlled trial to assess the effect of unconditional cash transfer on COVID-19 symptoms in residents of Ontario, Canada, who reported trouble affording basic necessities due to pandemic related disruptions.
Methods
Study design
This was an open-label randomised multicentre superiority trial with blind outcome assessors.
Participants
There was a single inclusion criterion that was based solely on patient report. To be eligible, participants had to report trouble ‘making ends meet’ or affording basic necessities due to COVID-19-related disruptions. We excluded individuals who were previously confirmed positive for COVID-19 based on laboratory testing or had symptoms consistent with COVID-19. Patients were approached during in-person or virtual clinical encounters at seven primary care sites in Ontario, Canada (population 14.6 million); there were six urban sites associated with St. Michael’s Hospital in Toronto and one in Manitoulin Island. We also recruited personal support workers, who generally earn a low income and come in close contact with clients, through an email notice distributed by employers.
Randomisation
Participants were allocated in a 1:1 ratio to either a cash transfer or control using web-based central randomisation in the REDCap electronic case report forms application. The allocation schedule was computer generated, stratified by centre and blocked using randomly permuted blocks of two and four.
Procedures
Participants randomised to the intervention group received an unconditional cash transfer of $C1000 or $C1200 for individuals living in households of three or more, via electronic transfer or bank draft. Both intervention and control group participants received information about reducing the spread of COVID-19 from the Public Health Agency of Canada over the phone and via email (see online supplemental appendix). After determining eligibility and randomisation, participants and care providers were aware of the allocated intervention.
Supplemental material
Outcomes
The primary outcome was the maximum count of symptoms consistent with COVID-19 over days 5, 10 and 14 as listed in the InFLUenza Patient-Reported Outcome (FLU PRO) instrument.15 A total of 32 items in six domains (nose, throat, eyes, respiratory, gastrointestinal and systemic) were scored as present or absent on each of days 5, 10 and 14; the highest symptom count recorded on a single day of days 5, 10 and 14 was used for analysis. The presence or absence of symptoms was recorded rather than symptom severity ratings that was required to analyse the originally specified continuous primary outcome of the maximum FLU PRO score over days 5, 10 and 14. This change to the primary outcome was made after data lock but before analysis of outcome data.
We added a secondary outcome deemed more specific for COVID-19, defined as the number of participants who met the case definition of probable COVID-19 as adapted from the US Council of State and Territorial Epidemiologists case definition of probable COVID-19 (see online supplemental appendix).16 Additional secondary outcomes were the self-reported number of close non-household contacts, PCR-confirmed COVID-19 based on nasopharyngeal swab, self-reported health, ability to make ends meet or afford basic necessities, food security and ability to afford medicines. The number of close non-household contacts was assessed on days 5, 10 and 14. All other secondary outcomes were assessed on day 14. We used a validated question to assess self-reported general health: ‘In general, how would you rate your health today?’. Possible responses were ‘very good’, ‘good’, ‘moderate’, ‘bad’ or ‘very bad’.17 18 To determine financial security, we used the following validated question: ‘At the end of the month, are you able to make ends meet?’.19 We used three validated questions to ask about food insecurity with three possible responses for each question: often true (worst food insecurity), sometimes true and never true (no food insecurity). As in previous food insecurity studies, responses of either ‘often’ or ‘sometimes’ were considered affirmative for food insecurity.20 Ability to afford medicines was assessed using one validated question about not taking prescribed medicines due to their cost, with participants being classified as adherent or non-adherent.21
Statistical analysis
The original sample size consideration was based on the maximum FLU PRO score as continuous primary outcome assessed across days 5, 10, 14. We required 176 participants per group to achieve 80% power to detect a difference in means of 0.21 on the FLU PRO, from 0.70 in the control group to 0.49 in the experimental group, at a two-sided alpha of 0.05, assuming an SD of 0.70 based on a previous study of individuals with influenza-like illness.15 Assuming 10% lost to follow-up, we recruited a total of 392 participants or 196 in each group. A sample size reconsideration for the new primary outcome using PASS Power Analysis and Sample Size Software V.15.0.10 (NCSS, Kaysville, Utah, USA) based on the observed mean count of symptoms of 1.94 in the control group indicated that the sample size of 392 participants would yield 90% power to detect a ratio of mean counts of 0.50, corresponding to a 50% relative reduction in symptom count, 82% power to detect a ratio of mean counts of 0.55, 71% power to detect a ratio of mean counts of 0.60, 59% power to detect a ratio of mean counts of 0.65 and 45% power to detect a ratio of mean counts of 0.70, corresponding to a 30% relative reduction in symptom counts, at a two-sided alpha of 0.05 after taking into account a 10% lost to follow-up. For all sample size considerations, the overdispersion parameter, defined as the ratio of the variance divided by the mean count, was set at 6.53, as observed in our data.
The primary analysis of the primary outcome was performed in the intention-to-treat (ITT) population, where patients who had at least one follow-up assessment at days 5, 10 or 14 days were analysed in the group they were randomly allocated to. We used bootstrapped Poisson regression analysis (1000 bootstrapped samples with replacement) to assess the superiority of the single unconditional cash transfer over control and expressed the treatment effect using between-group ratio of mean counts with 95% bootstrapped CI. In order to determine if results of the primary analysis were sensitive to the handling of missing data, we used both inverse probability weighting and fit a mixed-effects repeated measures model. Secondary outcomes were also analysed in the ITT population. Binary outcomes were compared between groups using risk differences with 95% CIs, and χ2 tests to derive two-sided p values. Count outcomes were analysed using rate ratios from quasi-Poisson models with 95% CIs and two-sided p values, which were adjusted for baseline values whenever available. Prespecified subgroup analyses of the primary outcome accompanied by tests of interaction were done according to age (<50 or≥50) and sex using bootstrapped Poisson regression. Finally, we conducted two sensitivity analyses of the primary outcome to assess robustness of results using inverse probability weighting in a quasi-Poisson regression analysis and a generalised Poisson mixed-effects model. Analyses were done in Stata V.15.1 (Stata) and R V.3.6.1 (R Foundation, Vienna, Austria).
Results
Between 20 April 2020 and 15 May 2020, we screened 491 potentially eligible individuals, and enrolled and randomly allocated 392, 196 to the cash transfer arm and 196 to the control arm, (figure 1). Two participants withdrew consent, both in the control arm (1%). Six participants in the cash transfer arm (3%) and 16 in the control arm (8%) were lost to follow-up.

Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
The trial population consisted of mostly women (67%) and most participants self-identified as either white (42%) or black (37%) (table 1). The average age was 44±12 years. Most participants (69%) had an income below $C30 000. In the cash transfer group, 115 (59%) had 2 or fewer household members and so received $C1000 while 81 (41%) participants had 3 or more household members and so received $C1200.
Baseline characteristics
When the trial started the number of new confirmed COVID-19 cases in Ontario (606 new cases per day, or 4 per 100 000 population) was near its first peak, and the rate of new confirmed cases later decreased but was sustained (above 294 per day, 2 per 100 000) during the study period. Closures of schools, child care facilities, some non-essential workplaces, restaurants, indoor and outdoor recreational facilities were enforced during the study period. Available governmental income supports included a $C2000 benefit every 4 weeks for some with an income disruption, and 35% (136) of participants reported receiving some COVID-19 income supports at baseline.
Effects of the interventions
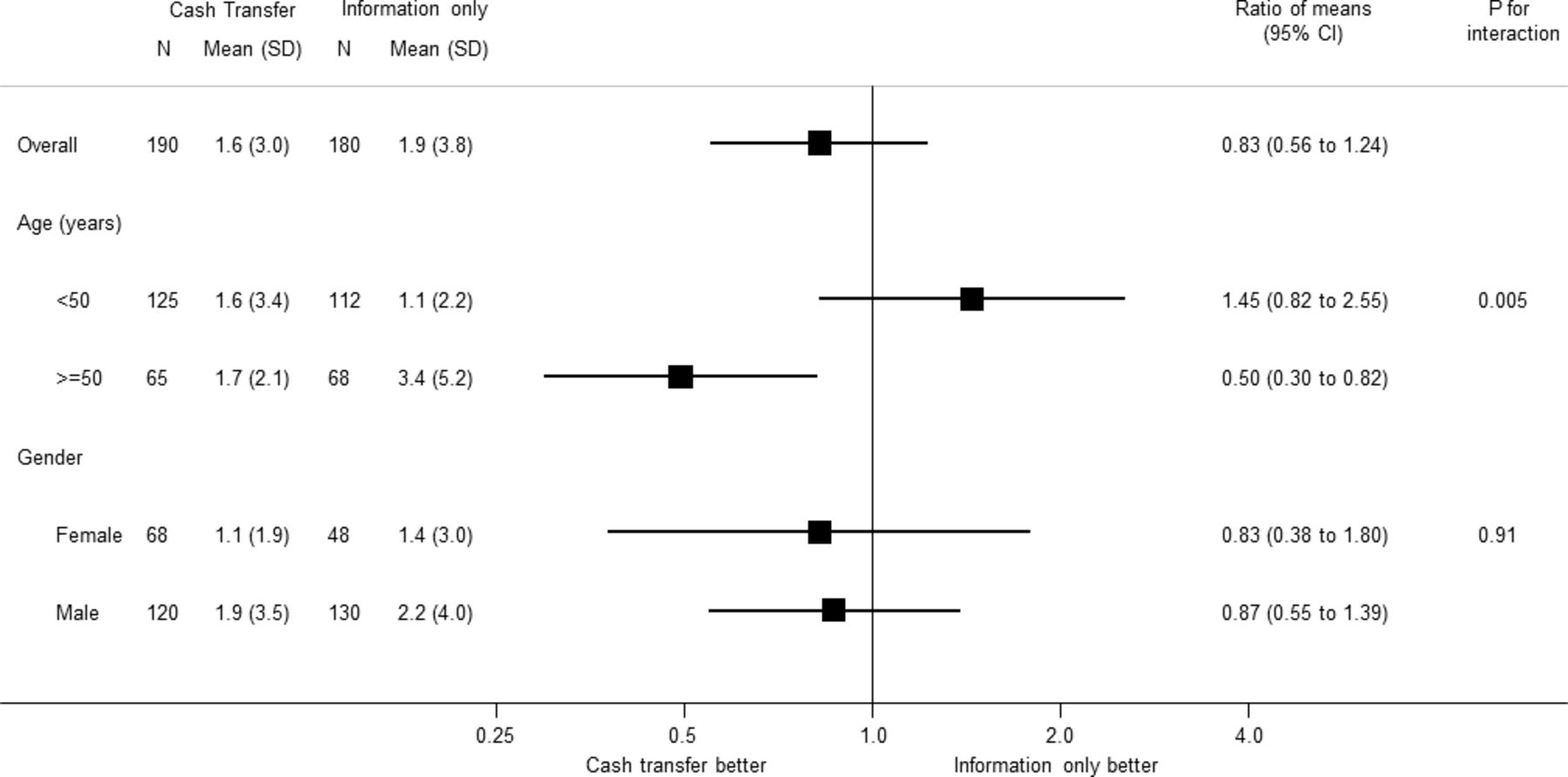
The cash transfer did not lower the symptom count up to 2 weeks (cash transfer 1.6±3.0 vs 1.9±3.8; ratio of means 0.83; 95% CI 0.56 to 1.24, p=0.34; table 2). Similar results were found when handling missing data using inverse probability weighting (ratio of means 0.84; 95% CI 0.56 to 1.24) and a mixed-effects model (ratio of means 0.83; 95 % CI 0.51 to 1.35). In prespecified subgroup analyses, there was no difference between females (ratio of means 0.83; 95% CI 0.38 to 1.80) and males (ratio of means 0.87; 95% CI 0.55 to 1.39) (p=0.91 for interaction), but cash transfers reduced the symptom count in those aged 50 years or older (ratio of means 0.50; 95% CI 0.30 to 0.82), but not in those <50 years (ratio of means 1.45; 95% CI 0.82 to 2.55) (p=0.005 for interaction; figure 2).
{kind=link}
{kind=link}
Prespecified analyses of the primary outcome.by age and gender
Outcomes
There were no statistically significant differences in secondary outcomes (table 2). There was no difference in the percentage of patients who met the clinical definition of probable COVID-19 (cash transfer 15/190 (8%) vs 23/180 (13%), risk difference 0.05 95% CI −0.11 to 0.01; p=0.12). Only one participant (0.5%) in the cash transfer and one participant in the information only group (0.6%) had PCR-confirmed COVID-19 during the study period. There was no evidence of a difference between groups in the number of close contacts outside of the household (mean number of non-household close contacts 3.5±5.9 vs 3.7±6.8; rate ratio 1.10 95% CI 0.83 to 1.46). General health did not differ between groups after 2 weeks (60% vs 63%). In both groups, around half of participants reported the inability to make ends meet or afford basic necessities at the end of the study (52% vs 51%). Optional comments made by participants indicated that many who reported the ability to make ends meet were only ‘barely’ making ends meet (see online supplemental appendix). Food insecurity was not reduced by cash transfers (80% vs 71%). Non-adherence to medicines due to financial reasons was relatively infrequent in the study population with no evidence for a difference between groups (11% vs 12%).
Discussion
In this randomised controlled trial, a cash transfer to financially vulnerable people during the pandemic neither reduced the primary outcome, symptom count up to 2 weeks, nor did it improve the secondary outcomes of general health or the ability to afford basic necessities. A prespecified subgroup analysis indicated that there might be a benefit of a cash transfer in those aged 50 years or older. The hypothesis that a cash transfer is beneficial in financially vulnerable people aged 50 years or older should be tested in future randomised trials.
There are at least four potential explanations for the lack of an observed benefit of a cash transfer in this trial: cash transfers may truly be unhelpful in this context, the risk of SARS-CoV-2 exposure may have been too low in the trial population to observe an effect of the intervention, the studied single cash transfer may have been insufficient, or a potential benefit in those aged 50 years or older was diluted or cancelled out by a lack of benefit or even harm in those aged less than 50 years. Factors other than financial security may be more important determinants of exposure to SARS-CoV-2 and adherence to physical distancing guidelines. Studies of cash transfers and ongoing income supports have generally found small benefits in some outcomes and no effect on other outcomes.13 14 Trust in government and other authorities is associated with adherence to physical distancing guidance.22 23 All participants were provided with information about physical distancing and respiratory hygiene and this reminder might have improved adherence.
Assuming that approximately 1 out of 10 cases was detected and confirmed by PCR during the study period,24 the risk of SARS-CoV-2 during the trial may have been around 5%. However, only one participant in each group had PCR-confirmed COVID-19, and our trial was not powered to detect differences in PCR-confirmed cases. Since there was an apparent benefit in participants 50 years or older, in whom symptom counts were larger than in younger participants, future trials could focus on older individuals, or individuals at even higher risk than those included in this trial.
The single cash transfer may not have provided sufficient financial security, and $1000 to $1200 may have been insufficient to substantially benefit participants. Work-related exposure to SARS-CoV-2 may not have been affected by a single cash transfer. Around half of participants reported the inability to make ends meet and most expressed concerns about food insecurity regardless of the cash transfer. This was true despite the fact that approximately one third of participants also received government supports (that were often worth $C2000 per month). The cost of living for a family of four in Toronto, Ontario, was estimated at $C3508 per month in 2018 and this is approximately equal to the combined value of the cash transfer in this study and the typical government support.25 The lack of an improvement in the ability to make ends meet in this study is notable because a trial of free medicine provision, that typically decreased expenses by less than $C200 per month, substantially improved the ability to make ends meet in a similar trial population.26
This is a rare trial of a non-pharmaceutical intervention during a pandemic conducted around the peak of new reported cases near the start of the pandemic. An evaluation of a single cash transfer programme in New York City during the pandemic indicated that the money was used to purchase basic necessities, but health outcomes were not assessed.27 We assessed both outcomes related to SARS-CoV-2 spread and outcomes related to personal and financial well-being.
This trial has several limitations. Trials of cash transfers cannot be blinded. The short study period meant that antibody testing would not be reliable, and it was not feasible to repeatedly test participants for presence of the novel coronavirus due to a limited supply of PCR testing when the trial was conducted. The sample size could have been insufficient to detect an important benefit; these trial results would ideally be pooled with results from similar studies. The primary outcome was based on symptom score developed for influenza and not COVID-19 although the symptoms are similar and we also employed a COVID-19 probable case definition. The long-term effects of a cash transfer cannot be determined based on a trial of a single cash transfer with a 2-week follow-up period. Results from a study in a high-income country with substantial social supports, including publicly funded healthcare services, should be applied with caution to other contexts.
Primary care providers can help ensure people have access to basic necessities by taking action at the individual patient, practice and community levels.28 Primary care providers can also use their knowledge of the challenges patients face to contribute to broader changes by leading or supporting studies that assess the effects of potential policy changes such as cash transfers that may promote health.
Conclusion
A cash transfer did not substantially reduce exposure to COVID-19 or improve the ability to afford necessities in a randomised controlled trial. These results indicate that the effects of cash transfers—that can represent substantial expense to governments—should be carefully assessed. The benefits might be greater in those at higher risk including those 50 years or older. To enable future pragmatic randomised comparisons, governments providing financial assistance could randomly assign some individuals to additional amounts geared to the cost of living while tracking outcomes to determine if financial supports have their intended benefits, such as allowing people to afford basic necessities.
Data availability statement
Data are available on reasonable request. The authors will disclose individual participant-level data on request after publication.
Ethics statements
Patient consent for publication
Ethics approval
The trial was approved by the St. Michael’s Hospital Research Ethics Board.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
PJ and BRdC contributed equally.
Collaborators DISTANSE COVID-19 (Direct Income SupporT and Advice Negating Spread of Epidemic COVID-19: a randomized controlled trial) study team: Yosra AlMakadma, Gordon Arbess, Michael Bedard, Kathryn Dorman, Tuan (Patrick) Hoang, Holly Knowles, Renata Leong, Danyaal Raza, Soruba Vijayaratnam, Itunu Adekoya, Oghenefejiro (Theresa) Ikpeni, Darshanand Maraj, Liane Steiner, Norman Umali, Hannah Woods, Aine Workentin, Kelly Anderson, Gary Bloch, Paul Das, Katie Dorman, Hannah Feiner, Amy Freedman, Johanna George, Abbas Ghavam-Rassoul, Rajesh Girdhari, Lauri Green, Charlie Guiang, Lindsay Herzog, Sue Hranilovic, Shelby Jaeranny, Tara Kiran, Bruce Kwok, Kyle Lee, Fok-han Leung, Jo Mellan, Eileen Nicolle, Jean Robison, Esther Rosenthal, Carly Ruderman, Vanna Schiralli, Celia Schwartz, Rami Shoucri, Ann Stewart, Alyssa Swartz, Thea Weisdorf, Lauren Welsh, Karen Weyman, Patricia Windrim, Karim Vellani.
Contributors NP made contributions to the study conception and design, literature search, data collection, analysis and interpretation, created the figures and drafted the manuscript; PJ and BRdC made contributions to the study conception and design, data analysis and interpretation, and drafted the manuscript. All authors revised the drafted manuscript critically for important intellectual content. All authors are accountable for all aspects of the work. NP accepts full responsibility for the work and the conduct of the study, had access to the data and controlled the decision to publish.
Funding The project was funded by support through the St. Michael’s Hospital Foundation (no grant number). The authors have full access and control of all primary data.
Disclaimer The funding sources played no role in the design, conduct, or reporting of the study. The authors have not entered into any agreement with the funder that may have limited their ability to complete the research as planned.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.