Article Text

Abstract
Objectives The COVID-19 pandemic has had an unprecedented impact across primary care. Primary care services have seen an upheaval, and more and more patients are engaging in telephone consultations in order to maintain social distancing. In the present study, we seek to quantify the effect of the pandemic on primary care prescribing.
Design We conducted a retrospective analysis of the English Prescribing Dataset from January 2014 to November 2020, totalling 7 542 293 921 prescriptions. Data were separated into prepandemic and pandemic sets. A Holt-Winters predictive model was used to forecast individual drug prescribing based on historic trends. Observed data were compared with the forecast quantitatively and qualitatively.
Setting All prescriptions signed in England and dispensed during the years 2014–2020.
Participants All residents of England who received a prescription from primary care facilities during 2014–2020.
Results Prescribing of numerous health-critical medications was above predicted in March 2020, including salbutamol (53.0% (99% CI (41.2% to 66.9%))), insulin aspart (26.9% (99% CI (18.5% to 36.6%))) and tacrolimus (18.6% (99% CI (8.3% to 31.1%))). Medications for end-of-life symptom control increased in April, including levomepromazine hydrochloride (94.7% (99% CI (54.6% to 163.0%))). Medications requiring face-to-face visits decreased, including the local anaesthetic bupivacaine hydrochloride (86.6% (99% CI (89.3% to 82.0%))). There was no observed change in medications relating to type 2 diabetes, hypertension or mental health conditions.
Conclusions Significantly increased prescribing of several medications was observed, especially among those critical for health. A dramatic spike in end-of-life prescribing highlights the adversity faced by community practitioners during 2020. Medications involving face-to-face consultations declined, as did contraceptives, travel-related vaccines and drugs used in dementia and Parkinson’s disease. Drugs relating to type 2 diabetes, hypertension and mental health were unchanged.
- general practice
- COVID-19
- public health
Data availability statement
Data are available on reasonable request. The data underlying this article are available from https://storage.googleapis.com/covid19-prescribing.jsfrazer.co.uk/home.htm.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key points
Question
How has prescribing and dispensing of medications by primary care practitioners been affected during the COVID-19 pandemic?
Finding
Prescribing and dispensing of a wide variety of medications was affected during the pandemic, including health-critical medications such as insulin and immunosuppressants, and end-of-life medications, while others involving face-to-face visits were reduced, and some including psychiatric medications remained unchanged.
Meaning
Our results highlight the adversities faced by primary care practitioners during the pandemic, particularly in the challenging area of increased end-of-life care being undertaken in the community as the pandemic progressed. These results also provide information on patient groups who have seen management of their health conditions altered during the pandemic and thus may require further support as lockdown eases.
Introduction
The United Kingdom’s National Health Service (NHS) relies heavily on primary care practitioners to assess patients with a multitude of presentations. In addition, they also commission services for patients, with development of a market system allowing general practitioners (GPs) to ‘buy’ specialist services from hospitals and other providers, encouraging competition in areas such as cost and waiting times.1 Almost 1 billion prescriptions were dispensed by GP practices in 2011, with a total cost of £8.8 billion (8.3% of the total annual budget of the NHS in this year).2
January 2020 saw the first mentions of COVID-19 in the UK press. Transmission increased through March, which also brought the UK’s first reported death,3 introduction of lockdown measures, closure of non-essential shops and services, and stay-at-home orders. Fatalities peaked in April, with a steady decrease in the following months until rising infections during September prompted the second national lockdown.4
The ongoing pandemic has dramatically changed approaches to primary care throughout the UK and abroad. Consultations are now increasingly conducted via telephone,5 bringing new challenges in clinical assessment and communication. In April 2019, 22 829 868 consultations were conducted in England and Wales, 14% of which were telephone appointments.5 By April 2020, the overall number of consultations had dropped to 15 835 467, although 48% were via telephone.6 This shift has seen mounting concern regarding the quality of telephone prescribing,7 8 although observational data is mixed.9 10 NHS approaches to chronic health conditions have also altered, with various delays in cancer care11 and elective surgery.12 Patient attitudes are similarly changing, with some individuals more hesitant to seek medical attention.13 14 Stockpiling of consumer goods, fuel, precious metals and even firearms has been reported in response to the COVID-19 pandemic.15 However, there is to date no peer-reviewed published literature investigating medication stockpiling, although some local media reports exist.16 17 Additionally, there is no peer-reviewed published literature to date to quantify the impact of COVID-19 on prescribing across a range of health conditions encountered by primary care prescribers. The present study aims to address this gap.
We hypothesised that national lockdown would lead to reduced patient interaction with primary care, and thus reduced prescribing for chronic health conditions such as hypertension, dyslipidaemia and type 2 diabetes mellitus. As symptoms of depression were shown to have increased during lockdown,18 we hypothesised an increase in acute antidepressant prescription. Additionally, we postulated that prescriptions for respiratory disease, such as inhaled bronchodilators and corticosteroids, would increase during this time due to possible medication stockpiling, and that dispensing of prescription paracetamol would be bolstered based on reduced availability of supermarket versions as a result of panic buying.19
Methods
We performed a retrospective database analysis on data extracted from the English Prescribing Dataset (EPD)20 from January 2014 to November 2020, totalling 71 months, and 7 542 293 921 prescriptions. The EPD catalogues all prescriptions signed in primary care practices in England and dispensed in England, Wales, Scotland, Guernsey, Alderney, Jersey and the Isle of Man, including all drugs, appliances and dressings.21 It contains data regarding the prescribing GP practices, as well as the quantity, strength and cost of items prescribed. Items prescribed in prisons, hospitals and the private sector are not included in the dataset. British National Formulary (BNF) chapters 1–19 were included in the analysis. No patient demographic data is included within the dataset, and numbers of prescriptions are given as aggregate data per GP practice for each month, and relate to prescriptions dispensed in that month. Thus, we were unable to control for potential biases relating to patient demographics, however, the aggregate nature of our analysis makes this unlikely to affect results. Prescriptions signed but not dispensed, signed outside of England, and prescribed and dispensed in hospitals, prisons, and private practice are excluded. The EPD is made available under the Open Government License V.2.0, and specific permission further to this was not sought.22
The data were separated into the pre-COVID (January 2014–October 2019) set for forecasting, and COVID-19 (November 2019–November 2020) comparison set, allowing validation of the model against several months of prepandemic data. For each month, the number of ‘items’ listed for BNF sections and individual drugs were summed, and time series formed for each. The EPD ‘items’ variable refers to ‘the total number of times that the medicine, dressing or appliance appeared on prescription forms that were prescribed and dispensed’.23 Seasonal decomposition of the time series using locally estimated scatterplot smoothing was used to decompose time series data into seasonal, trend, and irregular components, allowing easier pattern identification.24 Forecasting was performed using the Holt-Winters method, a predictive technique using triple exponential smoothing to apply moving averages to observed data. Triple exponential smoothing is an amalgamation of three separate smoothing methods: Simple Exponential Smoothing assumes that the data have no trend, producing a recursive average used as a baseline value to predict the next point; Holt’s Exponential Smoothing builds on the previous technique but also incorporates a trend component; Winter’s Exponential Smoothing includes a seasonal trend, which captures repeating time-based variation. These three components are weighted and combined, with exponentially decreasing weight given to older data points. Forecasts for each BNF section and drug were qualitatively compared with observed data by visual inspection of plots, and quantitatively compared using 99% forecast prediction intervals calculated via the R forecast function as described by Hyndman and Khandakar.25 Total UK death data (according to the Office for National Statistics26) was used to compare with prescribing trends for medications used in end-of-life care, with Spearman’s rho used to quantify correlation. Analysis was performed in R Studio V.1.3.959.27
Results
We analysed 107 BNF sections, and 1654 individual drugs. A small year-on-year increase in prescribing was noted, although total dispensed prescriptions in 2020 did not grossly differ in magnitude or seasonality from previous years. A mean of 90 871 011 dispensed prescriptions per month (SD 4 176 279) for our included sections was observed from January to November 2020. There was a decrease in prescribing during February each year (mean 7.94%, SD 3.47%), which then recovered in March, continuing normally. The number of dispensed prescriptions in March 2020 was 7.9% higher than the year mean monthly dispensed prescriptions. Throughout this section, we report dispensed prescriptions, and percentage difference relative to forecast data, unless stated otherwise. Further results can be accessed in online supplemental tables 2–4).
Supplemental material
Supplemental material
Supplemental material
Increased prescribing during COVID-19
Respiratory drugs
Prescribing of inhaled bronchodilators increased 41.5% (99% CI (31.3% to 53.5%)) compared with March 2020 predictions, dominated by terbutaline sulfate (64.3% (99% CI (45.1% to 89.3%))), salbutamol (53.0% (99% CI (41.2% to 66.9%))), ipratropium bromide (21.8% (99% CI (4.1% to 46.8%))), formoterol fumarate (15.2% (99% CI (2.7% to 31.3%))) and tiotropium bromide (12.3% (99% CI (0.3% to 27.6%))). Respiratory corticosteroid prescription was 39.8% (99% CI (30.3% to 50.7%)) above predicted for March, due predominantly to budesonide (37.3% (99% CI (25.7% to 51.4%))), inhaled beclometasone dipropionate (39.3% (99% CI (29.2% to 51.2%))) and inhaled fluticasone propionate (39.0% (99% CI (21.6% to 62.4%))) (figure 1, online supplemental table 1). Prescribing of pseudoephedrine was not affected.
Supplemental material
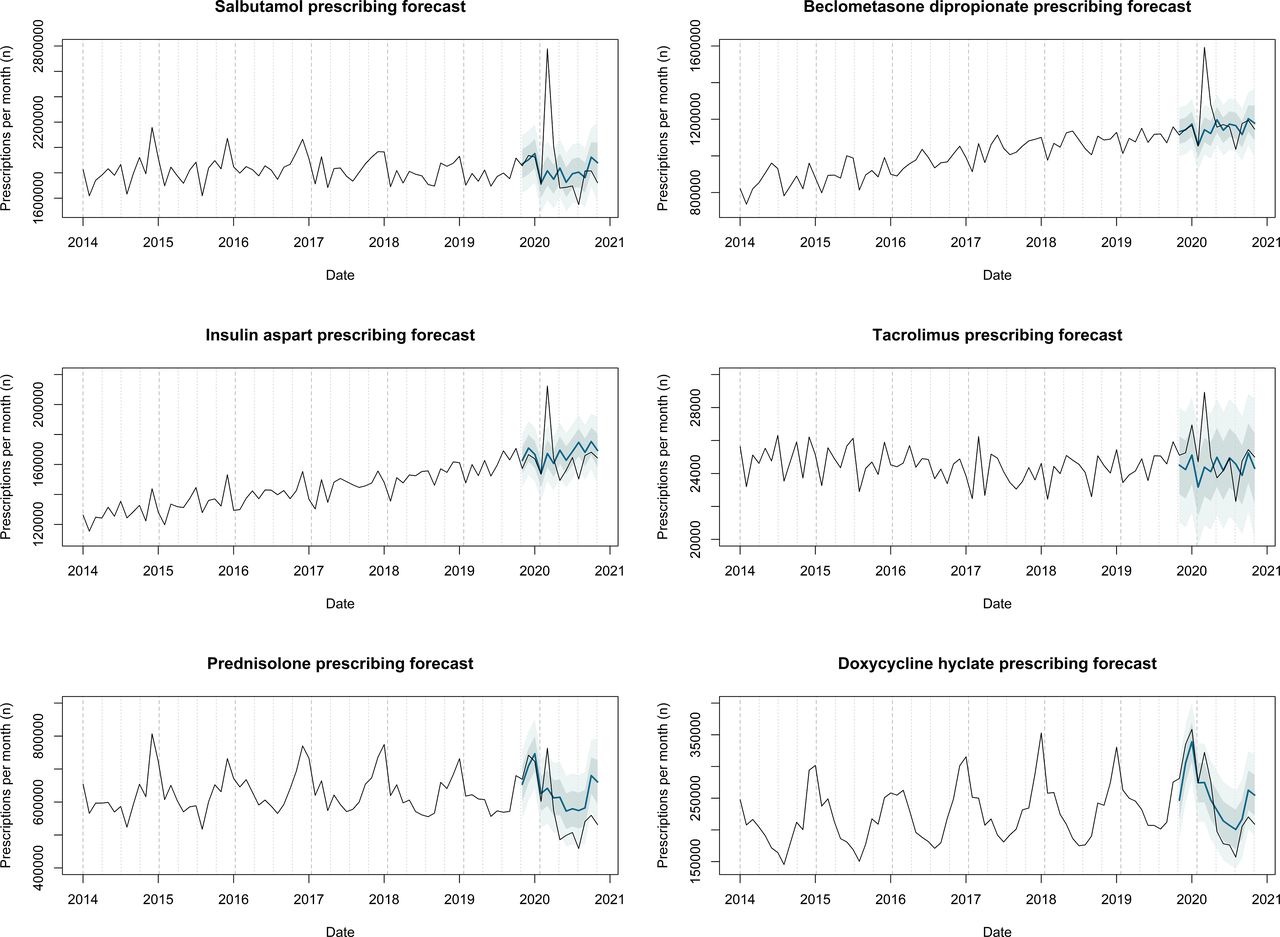
Medications with increased prescribing and dispensing during COVID-19. Number of prescriptions of particular medications issued by English primary care practices and dispensed over the period January 2014 to November 2020. Observed number of prescriptions is represented by a black line, with Holt-Winters forecast for October 2019 to November 2020 represented by a blue line. Prediction intervals are also displayed, with 95% prediction interval in dark grey, and 99% prediction interval in light grey. This figure displays a selection of medications which exhibited increased prescribing and dispensing during the COVID-19 pandemic.
Insulins and diabetic control
Increased prescribing of all types of insulin was observed during March 2020 (figure 1, online supplemental table 1); insulin aspart demonstrated the strongest increase from forecast (26.9% (99% CI (18.5% to 36.6%))), while glucose testing reagents (11.6% (99% CI (2.8% to 22.2%))), ketone testing strips (39.0% (99% CI (30.6% to 48.5%))), glucose (18.7% (99% CI (10.4% to 28.5%))), and glucagon (27.8% (99% CI (10.7% to 51.1%))) also increased. Glucose and glucagon both exhibited summer peaks.
Immunomodulators
Drugs used in the prevention of transplant rejection also exhibited a spike, with increases from March predictions observed for tacrolimus (18.6% (99% CI (8.3% to 31.1%))), sirolimus (16.2% (99% CI (−0.59% to 51.9%))), ciclosporin (14.0% (99% CI (−8.5% to 51.1%))), mycophenolate mofetil (12.8% (99% CI (4.8% to 22.2%))) and azathioprine (7.1% (99% CI (−0.2% to 15.6%))) (figure 1, online supplemental table 1). Similarly, the disease-modifying antirheumatic drugs hydroxychloroquine sulfate (13.1% (99% CI (3.8% to 24.1%))), methotrexate (8.4% (99% CI (0.8% to 17.2%))) and leflunomide (7.4% (99% CI (−0.7% to 17.0%))) all increased in March.
Benzodiazepines, opioids and analgesics
Prescribing of drugs associated with end-of-life care also reached their highest recorded point during 2020, coinciding with the UK peak number of deaths in April (figure 2). Prescribing of levomepromazine hydrochloride, midazolam hydrochloride, cyclizine lactate, haloperidol, and glycopyrronium bromide increased by 94.7% (99% CI (54.6% to 163.0%)), 78.0% (99% CI (53.1% to 112.4%)), 75.7% (99% CI (35.2% to 150.7%)), 36.5% (99% CI (13.8% to 70.5%)), and 17.2% (99% CI (0.1% to 41.4%)), respectively, in April (online supplemental table 1), and correlated strongly with total monthly deaths throughout 2020 (Spearman’s ρ=0.88, 0.93, 0.60, 0.48 and 0.58, respectively). Morphine sulfate and oxycodone hydrochloride increased by 7.5% (99% CI (−0.7% to 17.1%)) and 2.0% (99% CI (−5.3% to 10.5%)), respectively in April 2020, a small relative increase compared with their large absolute prescribing and dispensing volume. Paracetamol prescribing increased 21.7% (99% CI (8.6% to 38.5%)) during March 2020, although prescribing of ibuprofen was unaffected. Changes to prescribing of benzodiazepines were mixed, with an increase in prescribing of lorazepam relative to predicted in April 2020 (10.2% (99% CI (1.9% to 19.9%))), while diazepam, clonazepam and temazepam remained unchanged.

End-of-life care. Number of prescriptions of particular medications issued by English primary care practices and dispensed over the period January 2014 to November 2020. Observed number of prescriptions is represented by a black line, with Holt-Winters forecast for October 2019 to November 2020 represented by a blue line. prediction intervals are also displayed, with 95% prediction interval in dark grey and 99% prediction interval in light grey. This figure displays a selection of medications involved with end-of-life care during the pandemic. The bottom right panel displays total deaths during 2020, as well as prescribing of various medications used for symptom control at the end-of-life with peak and minimum prescriptions corrected to a scale of between 0 and 1 to allow comparison.
Decreased prescribing during COVID-19
Drugs requiring face-to-face visits
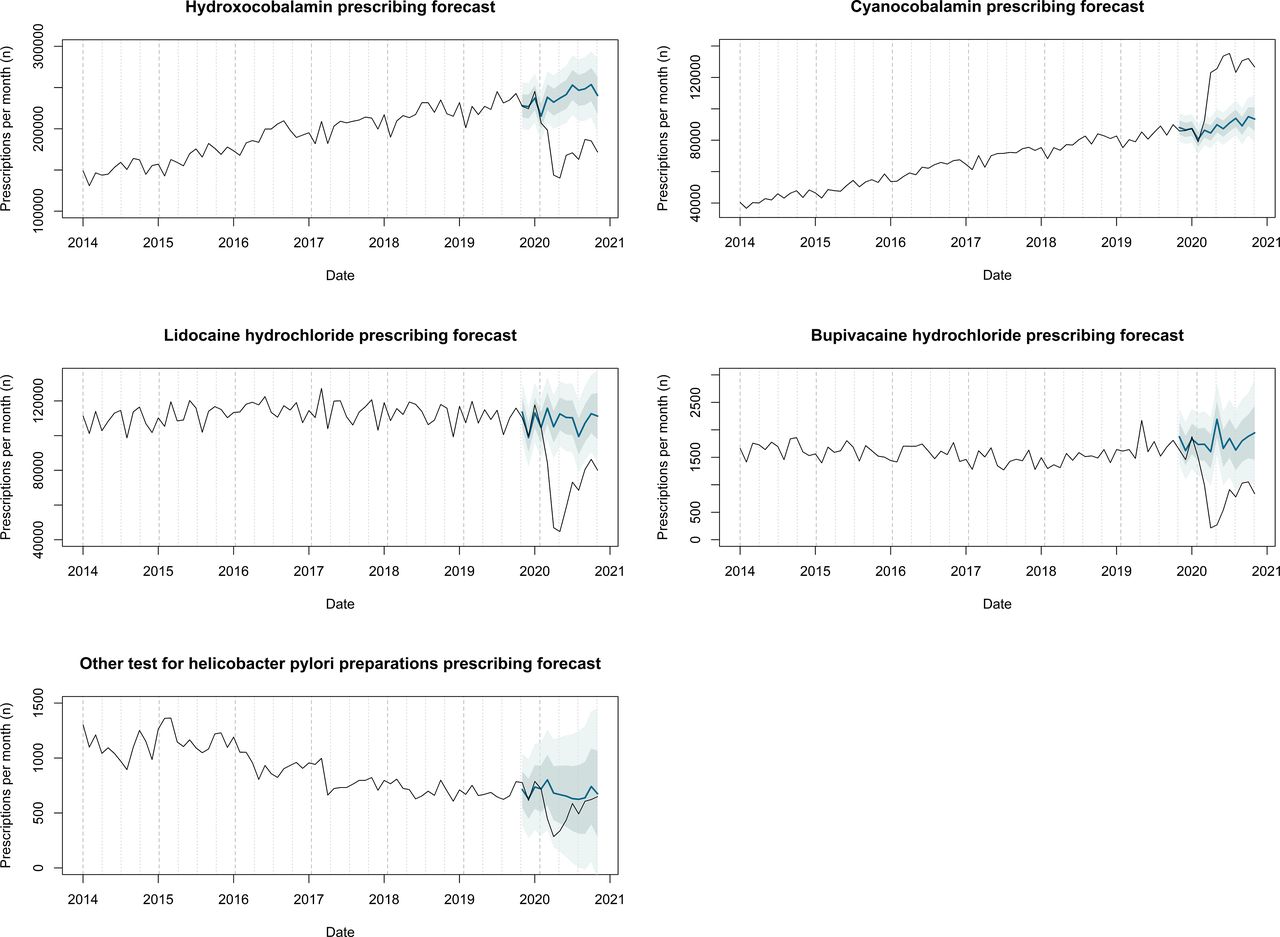
Medical devices and parenteral drugs reached a particularly low level of prescribing during the pandemic. Prescription of the intramuscular vitamin B12 injection hydroxocobalamin fell 38.0% (99% CI (−43.3% to –31.7)) in April 2020 (88 352 less prescriptions than predicted), while the oral form, cyanocobalamin, increased a corresponding 45.5% (99% CI (35.2% to 57.4%)) (38 489 more prescriptions than predicted). The local anaesthetics bupivacaine hydrochloride and lidocaine hydrochloride dropped by 86.6% (99% CI (−89.3% to –82.0%)) and 55.3% (99% CI (−59.9% to –49.5%)), respectively, in April, failing to recover even by late 2020 (figure 3). Helicobacter pylori testing preparations fell 44.1% (99% CI (−59.4% to –10.4%)) and 58.1% (99% CI (−71.6% to –20.2%)) in March and April, respectively, recovering by October. Prescribing of water for injection increased 80.1% (99% CI (58.8% to 108.0%)) from predicted in April, and urine testing reagents 70.0% (99% CI (45.2% to 104.5%)).

Medications involving face-to-face visits to primary care. Number of prescriptions of particular medications issued by English primary care practices and dispensed over the period January 2014 to November 2020. Observed number of prescriptions is represented by a black line, with Holt-Winters forecast for October 2019 to November 2020 represented by a blue line. Prediction intervals are also displayed, with 95% prediction interval in dark grey, and 99% prediction interval in light grey. This figure displays a selection of medications involving face-to-face visits to primary care. Hydroxocobalamin is an intramuscular preparation of vitamin B12, whereas cyanocobalamin is the oral alternative.
Steroids
Prednisolone prescriptions usually peak from December to January, reaching a trough in summer. During 2020, an unusual spike was observed in March (19.0% above predicted (99% CI (7.3% to 33.5%))), and the summer low point was exaggerated, with a 20.9% decrease relative to predicted in May (99% CI (−29.1% to –10.7%)) (figure 1). Prescribing of dexamethasone fell 21.6% from predicted in May (99% CI (−32.0% to –7.4%)).
Elderly care
Several drugs used in dementia (including donepezil, rivastigmine, memantine, and galantamine) exhibited a slight drop in absolute number of prescriptions dispensed during 2020, rather than the steady year-on-year increase they had been experiencing prior to 2020 (figure 4). Anti-Parkinsonian medications exhibited a similar decline (figure 4). Medications for nocturia and overactive bladder, including desmopressin acetate and tolterodine, dropped 16.8% (99% CI (−22.5% to –10.1%)) and 14.1% (99% CI (−20.7% to –6.3%)), respectively in May, as did lymphoedema (38.4% (99% CI (−43.1% to –32.8%))) and venous ulcer compression garments (32.3% (99% CI (−38.6% to –24.6%))).

Elderly care. Number of prescriptions of particular medications issued by English primary care practices and dispensed over the period January 2014 to November 2020. Observed number of prescriptions is represented by a black line, with Holt-Winters forecast for October 2019 to November 2020 represented by a blue line. Prediction intervals are also displayed, with 95% prediction interval in dark grey, and 99% prediction interval in light grey. This figure displays a selection of medications involved in elderly care whose prescribing and dispensing were altered during the COVID-19 pandemic.
Contraceptives
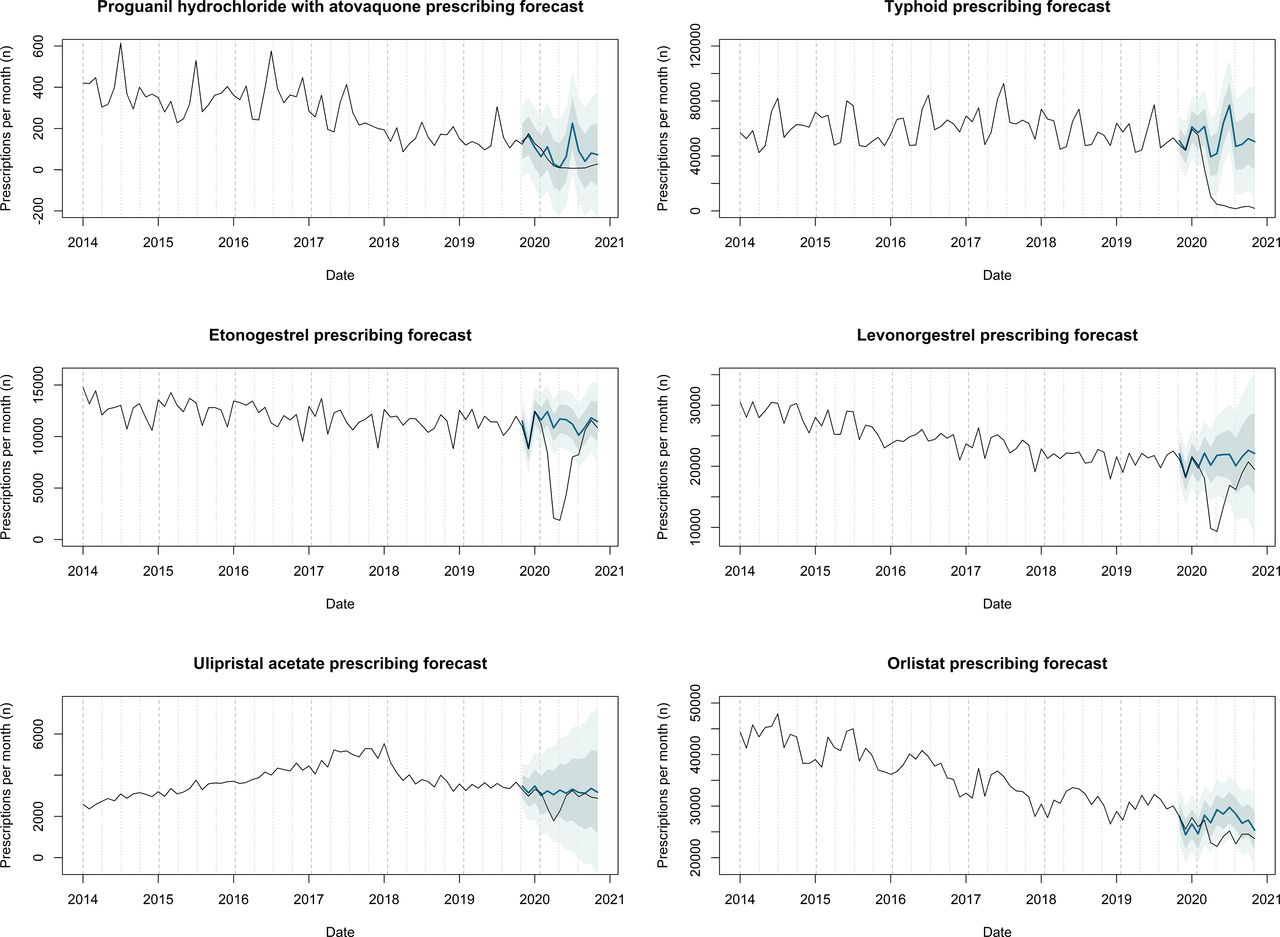
Contraceptives saw reduced prescribing throughout lockdown, reaching a low in May 2020 with a 19.5% reduction from predicted (99% CI (−25.8% to –12.1%)), dominated by levonorgestrel (57.2% (99% CI (−64.3% to –46.6%))), intramuscular medroxyprogesterone acetate (25.5% (99% CI (−31.3% to –18.7%))), and the subdermal implant etonogestrel (84.1% (99% CI (−86.2% to –81.1%))) (figure 5). Prescribing of the emergency contraceptive ulipristal acetate reached 41.5% below predicted in April (99% CI (−61.0% to –17.0%)). Vacuum pumps for erectile dysfunction had fallen by 48.2% in May (99% CI (−55.0% to –38.9%)), as had vaginal dilators (50.2% (99% CI (−61.3% to –30.0%))) and sildenafil for erectile dysfunction (19.8% (99% CI (−33.0% to –0.2%))). The usual summer peak in norethisterone prescribing was lost, reducing 45.9% in May (99% CI (−53.9% to –34.7%)).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Contraceptive, travel and weight loss medications. Number of prescriptions of particular medications issued by English primary care practices and dispensed over the period January 2014 to November 2020. Observed number of prescriptions is represented by a black line, with Holt-Winters forecast for October 2019 to November 2020 represented by a blue line. Prediction intervals are also displayed, with 95% prediction interval in dark grey, and 99% prediction interval in light grey. This figure displays a selection of contraceptive, travel and weight loss medications whose prescribing and dispensing was altered during the COVID-19 pandemic.
Vaccines and travel-related prescriptions
The summer spike usually associated with proguanil hydrochloride with atovaquone was not observed, with a 96.9% reduction from predicted in July 2020 (99% CI (−98.2% to –88.6%)). The typhoid vaccine, usually peaking in January and June, dropped by 50.3% in March (99% CI (−61.3% to –30.6%)), and never recovered throughout the usual summer peak season, with a 96.7% reduction in July (99% CI (−97.4% to –65.4%)) (figure 5). Diphtheria, cholera, yellow fever, hepatitis A, hepatitis B and combined vaccines all exhibited similar trends. Influenza and pneumococcal vaccines were not affected, however, and their absolute number was not different from previous years. In fact, their uptake was slightly increased by late 2020; the influenza vaccine experienced a 44.1% increase in September (99% CI (2.2% to 144.4%)) and 20.7% increase in October (99% CI (1.4% to 49.0%)), with the pneumococcal vaccine increasing 53.8% (99% CI (2.6% to 207.3%)) and 45.2% (99% CI (16.5% to 92.6%)) for the same months, its most successful year since 2014.
Obesity and substance dependence
Prescribing of the antiobesity drug orlistat usually peaks in May–June each year. This seasonality was absent during 2020, with a 24.3% reduction in May (99% CI (−33.2% to –12.8%)) (figure 5). Changes in drugs associated with substance dependence were mixed; prescribing of some medications for opioid dependence was increased, with methadone hydrochloride and buprenorphine hydrochloride 15.3% (99% CI (5.4% to 27.3%)) and 19.7% (99% CI (11.7% to 28.8%)) above April predictions, respectively. Drugs used in the treatment of alcohol dependence increased only slightly. Nicotine decreased 13.5% in April (99% CI (−36.8% to 36.9%)), although this was not statistically significant.
Drugs unchanged during COVID-19
With the exception of a small spike in March 2020 which quickly returned to baseline, antihypertensives were not significantly affected by the pandemic, nor were antianginals, anticoagulants, antiepileptics, oral antidiabetic drugs, antidepressants or antipsychotics (online supplemental tables 1–4).
Antibiotics
While prescribing of the antibiotics class was not significantly different from prediction, some intraclass differences were observed. Prescribing of phenoxymethylpenicillin, typically indicated for childhood throat infections, peaked as usual in March, but subsequently fell by 33.0% (99% CI (−43.6% to −17.5%)) in April, maintaining a reduced level of prescribing throughout 2020. Chloramphenicol experienced a similar abrupt end to its usual Spring peak. Prescribing of doxycycline hyclate spiked in March with a subsequent decrease below expected in summer (figure 1). Prescribing of flucloxacillin sodium was 12.7% (99% CI (−23.1% to 1.0%)) lower than July prediction, with a similar trend for the acne antibiotics neomycin and lymecycline.
Discussion
Primary care prescribing has profoundly changed during the COVID-19 pandemic. Increased prescribing and dispensing of medications used in chronic obstructive pulmonary disease (COPD), insulin-dependent diabetes, and transplant immunosuppression was observed, while drugs involving face-to-face visits were avoided. Elderly care medications, including anti-dementia drugs and those used in the treatment of Parkinson’s disease, experienced an alteration of their upwards trend towards a decline during the pandemic. Somewhat surprisingly, the majority of drugs associated with chronic health conditions such as hypertension, type 2 diabetes and mental health conditions, were not grossly affected.
Our results indicate increased prescribing and dispensing of health-critical drugs during the initial pandemic months. Affected medications include insulins, transplant immunosuppressants and respiratory drugs such as inhalers (figure 1). Since prescriptions of these medications increased during March and April 2020, returning to normal thereafter, we surmise that that the observed stockpiling of consumer goods translated into medication stockpiling.15 We theorise that patients anticipated shortages of medications and reduced ability to attend GP practices, and so were motivated to request prescription of extra medications, or seek dispensing of already prescribed items. A survey of solid organ transplant recipients in Germany highlighted this group’s particular fears regarding COVID-19.28 Montelukast deviated minimally from prediction, as did the beclometasone/formoterol fumarate combination inhaler, suggesting that these trends may be driven by patients with COPD, rather than asthma. The observed increased prescribing and dispensing of prednisolone and doxycycline, commonly used in COPD rescue packs (a ‘pack’ containing a combination of steroid and antibiotic kept by the patient and used in the event of a COPD exacerbation), supports this hypothesis. Indeed, patients with COPD are particularly at risk of mental health disorders in response to lockdown.29 The possible difference between patients with COPD and asthma is interesting, as UK shielding guidelines were similar for both patients with severe COPD and severe asthma.30 Prescribing of oral diabetic medications did not significantly differ from forecast, suggesting that medications for individuals with type 1 diabetes, for whom abstinence from insulin would be most detrimental, are responsible for the spike in insulin and testing prescriptions. Insulins were reportedly stockpiled in response to the proposed UK exit from the EU in 2019,31 although we find no evidence of increased prescribing and dispensing of insulin during that time. Prescribing and dispensing of both glucose and glucagon increased in March 2020, and their observed annual summer prescribing peak is consistent with previous reports.32 33 Possible alternative explanations for increased prescribing and dispensing during the lockdown period include increased GP prescribing, or increased dispensing by patients’ pharmacies when attempting to fulfil prescriptions, although to our knowledge there is not yet any peer-reviewed evidence to support this theory.
The alarming spike in palliative care medication prescription coincided with the UK peak overall deaths. National Institute for Health and Care Excellence (NICE) guidelines for management of COVID-19 at the end of life specifically recommends levomepromazine for control of delirium or agitation,34 which has been borne out in observed community prescribing (figure 2). A recent survey of practitioners regarding provision of end-of-life care highlights the unprecedented demand on the service.35 Further to the high death toll among the elderly, their overall care appears to have suffered throughout 2020, with several drugs used in the management of dementia and Parkinson’s disease exhibiting a reduction in absolute number of prescriptions dispensed in 2020, rather than the steady increase they had been experiencing prior to this. This correlates with the observed lack of new diagnoses of dementia,36 37 with the attrition possibly reflecting patient deaths, as treatment with drugs to combat Parkinson’s disease and dementia is often lifelong. It may also be possible, however, that elderly patients were unable to visit pharmacies to have their prescriptions dispensed due to reduced social support from relatives during lockdown, shielding advice or fears of leaving the house.
Prescribing of drugs involving face-to-face visits reduced during the pandemic, including intramuscular injections, contraceptive implants, practice-based diagnostic tests, and local anaesthetic agents. This is in line with the observed dramatic decrease in face-to-face consultations recorded during 2020.6 The depot antipsychotic medications were an exception, likely due to their enforced administration under the mental health act. Despite guidance advising switching patients from warfarin to direct oral anticoagulants (DOACs) in order to minimise clinic visits,38 and a preprint study reporting that 12.2% of patients taking warfarin in England were switched (most commonly to edoxaban or apixaban) between March and May 2020,39 we detected no significant deviation from prediction in prescribing of warfarin or DOACs during 2020. The aforementioned study includes only 40% of England’s population, and does not appear to include dispensing data, possibly accounting for these discrepancies.
Despite the considerable attention hydroxychloroquine received as a potential COVID-19 therapy, other antirheumatic drugs exhibited a similar degree of increased prescribing. One explanation of the observed increase is its use in chronic health conditions rather than to perceived benefits against COVID-19, although perhaps reduced availability of hydroxychloroquine due to diversion for COVID-19 therapy resulted in increased switching to alternatives. Indeed, prescribing of dexamethasone fell during COVID-19 despite widespread publicity of its benefit,40 possibly as a result of fewer new cancer diagnoses, or possibly due to supply issues in primary care with increase hospital demand for the drug.
A reduction in transmissible childhood diseases (including measles, mumps, rubella, scarlet fever and whooping cough) has been reported during 2020.41 Similarly, we observed a reduction in prescribing of antibiotics commonly used to treat common bacterial illnesses in children, including phenoxymethylpenicillin; we surmise that this is due to reduced overall social contact among children, including national lockdown, as well as shop and school closures, although this is an area in which much further work is needed to ascertain whether transmission was indeed reduced, or healthcare-seeking behaviour was curbed. While there are concerns that telephone consultation is leading to a generalised overuse of antibiotics in primary care, this is not apparent among our results.42 Due to widespread travel restrictions, prescribing of travel-related vaccines and medications fell dramatically. Norethisterone has a summer-predominant seasonality, thought to reflect attempts to avoid periods during travel,43 which was lost during 2020.
Prescribing of orlistat exhibits an almost 25% increase in prescribing in summer compared with winter, although this peak was almost completely lost during 2020. To our knowledge, this seasonality has not been described previously, and does not appear to coincide with peak dieting motivation,44 45 calorie intake or seasonal exercise.46 Colchicine also displayed seasonality, in agreement with preprint data regarding the summer-predominance of gout.47 There was a slight peak in nicotine prescribing during January, in agreement with published data.48
No antidepressant deviated significantly from forecast at any point in 2020. This likely multifactorial, and is is at odds with our prespecified hypothesis. Indeed there has been a reported reluctance for patients to attend primary care for mental health concerns,49 while a clear increase in symptoms of depression has been described,18 and intentional drug overdoses have spiked during COVID-19,50 51 betraying a further deterioration in general mental health. While there is some suggestion that patients are increasingly avoiding antidepressant medications due to publicised withdrawal effects,52 patients experiencing low mood as a result of lockdown may be facing delayed diagnosis, and likely represent an underserved group during the pandemic, thus reducing access to comprehensive investigation of physical causes of low mood, and to first-line treatments such as cognitive behavioural therapy.
Our results reveal the effects of several recent medication approvals and withdrawals. Prescribing of ranitidine dropped by 99.6% in August 2020, following its suspension in mid-2019 due to a carcinogenic ingredient.53 This was offset by an increase in famotidine and cimetidine. Prescriptions of ingenol mebutate fell 99.6% by August 2020 due to its suspension by the European Medicines Agency in the previous February.54 Prescription of the subcutaneous glucagon-like peptide-1 agonists fell gradually during 2020, possibly due to the recent approval of oral semaglutide.55
What this study adds
Our analysis provides some of the first published quantifiable impact of COVID-19 on primary care prescribing, and further adds to existing evidence regarding the impact of the pandemic on both acute and chronic health conditions. We observe trends in increased prescribing and dispensing of multiple medications relating to health-critical conditions, and present mediation stockpiling as possible explanation of these results, with others including altered GP prescribing or pharmacy dispensing habits. This research reveals issues surrounding reliance on in-person healthcare visits, which may discourage compliance or invoke fear among patients, thus highlighting societal groups who may experience disproportionate detriments in care during lockdown. Overall, however, measures taken by primary care practitioners to maintain prescription of medications for long-term health conditions, such as increased electronic repeat prescribing,56 57 appear to have been successful.
Strengths and limitations
We analysed an extensive dataset including dispensed prescriptions from the whole of England over the 6 years prior to the COVID-19 pandemic. Our forecast overlapped with several months of prepandemic data, thus validating the model. However, due to the volume of data analysed, we were unable to offer comparison of alternative forecast models. One major limitation of our study is that it does not fully elucidate patient attitudes to their health conditions; only information regarding dispensed prescriptions is captured, and not patient compliance with prescribed medications. In addition, we do not have data regarding absolute disease incidence, thus it is not clear from our data whether changes in number of prescriptions represents changing incidence of certain conditions during the pandemic, or simply a reluctance to interact with healthcare professionals for diagnosis. Due to the limitations of the dataset, we were unable to draw conclusions regarding differential prescribing by patient group during the pandemic, although were able to make some limited inferences based on the class of drug prescribed, for example, those drugs commonly used in paediatric populations or in elderly care.
Conclusion
Our results highlight the disruption experienced by primary care prescribers during the COVID-19 pandemic. Prepandemic levels of prescribing and dispensing were observed for chronic health conditions such as type 2 diabetes and hypertension, although there were clear reductions in prescribing for Parkinson’s disease and dementia. Increased prescribing and dispensing of health-critical medications was observed. Medications relating to mental health were not significantly affected. Strains on community services are underscored by the dramatic increase in end-of-life care prescribing. Thus, the above data highlights those particularly vulnerable patient groups who may benefit from future specific care campaigns. Further work will involve reassessment of trends following a period of lifted lockdown to investigate how long-term prescribing is recovering.
Data availability statement
Data are available on reasonable request. The data underlying this article are available from https://storage.googleapis.com/covid19-prescribing.jsfrazer.co.uk/home.htm.
Ethics statements
Ethics approval
Ethical approval was not required as this study makes use of fully anonymised retrospective data.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JSF conceived of the study, conducted data analysis, wrote the first draft of the manuscript, provided details regarding clinical aspects of the study, and provided critical review. GRF was involved with the design of the study, conducted data analysis, wrote the first draft of the manuscript and provided critical review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.