Article Text

Abstract
The primary purpose of this article is to provide family physician researchers interested in conducting a qualitative research study a concise guide to the analysis. Drawing from approaches outlined in popular research methodology textbooks and employing an exemplar from a minority health disparities research study, this article outlines specific steps useful for researchers and practitioners in the field of family medicine. This process of qualitative data analysis is situated within the larger framework of qualitative research to better position those new to qualitative designs to more effectively conduct their studies. A 10-step process useful for guiding qualitative data analysis is provided. The 10 steps include (1) assembling data for analysis, (2) refamiliarising oneself with the data, (3) open or initial coding procedures, (4) generating categories and assigning codes to them, (5) generating themes from categories, (6) strategies of validation, (7) interpreting and reporting findings from the participants, (8) interpreting and reporting findings from the literature, (9) visual representations of data and findings, and (10) strengths, limitations, delimitations and suggestions for future research. This work provides clear and accessible guidelines for conducting qualitative data analysis for emerging researchers that is applicable across a wide array of topics, disciplines and settings.
- qualitative research
- family medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Significance statement
Historically viewed as a soft alternative to what many scholars consider more scientifically legitimate quantitative approaches, qualitative research continues to gain ground in both stature and application across disciplines. Although there are parallels between quantitative and qualitative methodologies in design and implementation, qualitative research has its own unique characteristics, underlying assumptions and modus operandi that distinguish it from other forms of research. Considered the most elusive task in a qualitative research project, data analysis can be challenging to both novice and experienced researchers. Drawing from approaches outlined in popular texts and employing an exemplar from the Minority Health Disparities Study, an accessible 10-step approach to qualitative data analysis to guide qualitative researchers in the field of family medicine is advanced.
Introduction
This article begins by offering a definition, characteristics and brief history of the origins and development of qualitative research to better position this analysis. This work can be used to inform the qualitative data analysis procedures for researchers who use a mixed-methods survey,1 semistructured interviews,2 case study research3 and other qualitative approaches. Key components of a qualitative research design are also outlined to situate qualitative data analysis within the larger framework of this form of enquiry. This is followed by a succinct overview of the process of qualitative data analysis as presented in several contemporary research methodology textbooks. Drawing on procedures advanced in these works, and my own research as part of an interdisciplinary team at a large, research-intensive institution, a 10-step approach to qualitative data analysis is presented to guide those interested in using qualitative research in family medicine.
A background to qualitative research in the social and health sciences
Characteristics of qualitative research
Qualitative research can be defined as an umbrella term used to designate a family of approaches that emphasise inductive reasoning, collecting data in natural settings and understanding participants’ points of view. Qualitative researchers use interviews, participant observation, document analysis and so on to generate patterns or themes to describe and explain phenomena in depth. Other terms describing this type of research are naturalistic, ethnographic, interpretive and symbolic interactionist.4 In addition to inductive data analysis, long-term immersion of the researcher in naturalistic settings, and thick and rich description,5 other characteristics delimiting qualitative research include the researcher as the primary data collection instrument, an overarching concern with process, an emphasis on emergent and flexible design, non-random purposeful sample selection, and a holistic understanding fostered through collection and analysis of multiple forms of data and perspectives.4 6–8 Qualitative researchers aspire to shift the mantle of authority from the investigator to the participant, the latter viewed and purposefully selected as the expert on the central phenomenon of study and therefore assuming more status and a greater role in the research than historically accorded by more paternalistic forms of quantitative enquiry. Conceptualised in this manner, the qualitative researcher has the means to get closer to the participants and topic of enquiry than that afforded by quantitative designs.
The origins and history of qualitative research
The origins of qualitative research are traced to the early 20th century to the pioneering ethnographic fieldwork of anthropologists studying non-Western cultures who emphasised a holistic understanding achieved through participant-centred analyses involving immersive fieldwork, learning the language and the culture of participants, and collecting multiple forms of data. Interpretive forms of enquiry continued to gain momentum with the work of ‘Chicago School’ sociologists9 who borrowed their methods from these anthropologists and applied them to study a wide range of social phenomena.9 10 These social scientists laid the foundation for what Denzin and Lincoln11 12 referred to as the Modernist or Golden Age and Blurred Genres (1950–1980) phases of qualitative research that signalled the beginning of the qualitative revolution13–15 that would forever change the research landscape. Table 1 lists the iconic publications marking this qualitative revolution. More recently, this tradition has been built on and extended by well-known qualitative researchers such as Norman Denzin, Yvonne Lincoln, Kathy Charmaz, John Creswell and other scholars representing a wide range of disciplines in the social and health sciences. I direct the reader to Denzin and Lincoln’s Handbook of Qualitative Research as an informative resource for budding qualitative researchers in family medicine.16
Iconic publications marking the qualitative revolution in the social sciences5 20 27 34–38
Designing a qualitative research study
Contemporary scholars typically view the process of designing and conducting qualitative research as iterative or cyclical in that data collection and analysis are simultaneous activities. The research design—the overall plan of the research study—should be analytically congruent with all pieces fitting neatly together throughout design, implementation and analysis phases. Box 1 presents a qualitative research design procedural checklist adapted from the various publications of John Creswell and associates, as well as from my own teaching and research employed in a battery of research methods courses across disciplines and colleges at my host institution.7 17–19 As shown in Box 1, the title in a qualitative research study should represent the qualitative design used and state the topic being explored. The introduction serves to introduce the focus of the study, the theoretical framework driving it, and relevant literature and the gap that the proposed research will fill. This sets the stage for the purpose statement, historically considered the most important component of the entire study7 19 which should succinctly state the overall goal or purpose of the research and the specific qualitative approach employed (eg, grounded theory, ethnography, narrative and so on). The purpose statement is followed by the central or ‘grand tour’ question20 consistent with the purpose statement, the overall goals and rationale of the study, and its subquestions that break the central question into more manageable parts.
Qualitative research design procedural checklist
Title (reflect the qualitative design used and communicate the central focus of the study).
Abstract (tight, succinct and comprehensive).
Table of contents (for theses and dissertations, not published research articles).
Introduction and identification of the research problem or problem statement (what is the topic, why it is an important topic to study, why the study is needed, theoretical framework and so on).
Qualitative purpose statement.
Qualitative research central and subquestions (consistent with the goals and rationale of the study, feasible, well written, succinct and analytically congruent).
A concise summary of relevant literature and how and where it is used in the study (consistent with the goals and rationale of the study).
Researcher positioning/reflexivity (worldview, theoretical lens and approach).
Definition of terms (clearly define terms and concepts used in the study).
Rationale for why qualitative research was selected (over quantitative or mixed methods).
Rationale for choice of qualitative approach and subapproach used and why.
Institutional review board and ethical considerations (identify permissions that have been granted) and include ethical considerations or issues that were taken into account in the design of this project.
Sample selection procedures documented and explained (include number and demographic information of participants, how participants will be recruited and how they will benefit from the study; also provide site selection criteria and so on).
Data collection methods documented, justified, designed and implemented. Multiple forms of data used as one form of triangulation.
Data analysis methods justified, documented and implemented (indicate data coding and analysis procedures, use of software, multiple coders, validation strategies, triangulation and so on).
Discussion and presentation of research findings, results and conclusions. What emerged (narratives, models, themes, theory and so on)? Use of visual representations (tables, graphs, figures, diagrams, flow charts), comparisons with other research, implications for research and practice, strengths and limitations, suggestions for future research.
References cited pages.
Attached data collection instruments and samples of data analysis (eg, coding and so on).
Samples of each kind of data collected.
Other components of a qualitative research report include a concise summary of the relevant literature included in several key sections of the manuscript, usually placed in the introduction, statement of the problem, findings and conclusions sections. In qualitative research, the investigator typically positions oneself in the research process outlining her or his worldview, theoretical lens and stated biases of the research. As in all research, the author should clearly define key terms and how they are used in the study, a rationale for why qualitative research was selected over quantitative or mixed-methods research, the type of qualitative research design and subapproach selected and why, as well as information regarding institutional review board and ethical considerations and permissions granted from sponsoring agencies to conduct the research. Sample selection procedures need to be documented and explained that specify why and how participants and sites will be chosen and how participants will reciprocally benefit from the study. Data collection procedures and protocols should be documented, designed and implemented. The process of coding and data analysis needs to be clearly outlined along with the discussion and presentation of the research findings (eg, categories, themes, models and theories), conclusions, strengths, limitations and suggestions for future research, references cited pages, and other materials such as data collection instruments included in the appendices.
The process of data analysis in qualitative research
The process of data analysis in qualitative research is considered the most challenging aspect of a qualitative study, often viewed as a personal journey learnt partly through one’s training and partly through repeated practice. There are few universally agreed on procedures or techniques to guide researchers new to qualitative research. As a result, qualitative researchers commit intensive time to learn, conduct and hone their data analysis skills as they become more proficient in this area.
Turning to research methods texts that I use in several research courses for the purpose of training graduate students in qualitative methodology, each presents workable variations on this process and provides suggestions as to how proceed.7 8 19 21 22 Drawing from Glaser and Strauss’ (1967) The Discovery of Grounded Theory,23 Merriam and Tisdell recommend an inductive and comparative strategy to make sense of the data to answer one’s research question(s).8 They provide a step-by-step process of qualitative data analysis (table 2). Creswell and Poth7 note several commonalities in qualitative analysis procedures ‘across many books on qualitative research’ (p183) that include preparing and organising data for analysis, coding and condensing codes to reduce the data into themes, and representing the data in figures, tables and narratives. These authors visually organise their steps of qualitative data analysis through a ‘data analysis spiral’ (p185–186), and outline additional procedures they deem necessary depending on which of five popular contemporary approaches (ie, narrative, phenomenology, grounded theory, ethnography and case study) is used.7 Creswell and Guetterman19 also outline six steps for analysing qualitative data, whereas Marshall and Rossman22 present a seven-phase analytical procedure.
Steps of qualitative data analysis as outlined in four popular textbooks7 8 19 22
The Minority Health Disparities Study
In my own research, I have used different data analysis techniques depending on the research question and goals of the research. For purposes of this paper, I have selected a research project where I was a member of an interdisciplinary team charged with identifying strategies for healthcare workers to better use research to improve practice in the area of minority healthcare at a large Midwestern research-intensive university (Babchuk WA, Brand LL, Guetterman TC. Improving research-based practice through qualitative inquiry: a community-based study of minority health care. In preparation, 2019). Employing a collaborative, community-based qualitative methodology, we interviewed 13 healthcare workers using a semistructured interview protocol and analysed data through our own evolving procedures. We implemented our own modified data analysis procedures presented in table 3, many of which overlap with steps from the text presented in table 2. This study will be used here as an exemplar to better illustrate these 10 steps.
Ten steps and procedures for conducting qualitative data analysis
Step 1
As shown in table 3, Assembling materials for analysis is the first step in qualitative data analysis by which the researcher transcribes interviews and lays out other forms of data to be analysed (eg, observational notes, memos and so on). It is important that researchers organise data in a manner meaningful to them, and that data are clearly labelled and stored in a password-protected computer and/or locked filing cabinets. Once transcribed, interview transcripts should have margins on the left and right sides of the text for coding, particularly when using hand-coding techniques. Participant observation protocols typically include a left column for descriptive notes and a right column for reflective notes used together in the analysis often to bolster or triangulate findings from the interview data.19 As the primary form of data collection was interviews in the Minority Health Disparities Study, these were transcribed verbatim and printed with margins on both sides of the text for the hand-coding we would undertake.
Step 2
Refamiliarising oneself with the data constitutes an initial read through the transcripts and/or notes from participant observation, documents and so on, and is conducted to bring the researcher increasingly closer to the data. The researcher should begin or continue writing personal reflective field notes, hunches, thoughts and so on throughout the various steps of qualitative data analysis. A technique developed by the early anthropological fieldworkers, Glaser and Strauss23 labelled this process memoing, and it is an important and widely employed strategy used to help guide the emerging analysis in qualitative research.23 In the minority health disparities research study, we read through the interview transcripts and made notes in the margins before we began coding to become more familiar with our data. This was augmented by ongoing researcher team meetings where we discussed our collaborative analysis.
Step 3
For open or initial coding procedures, the researcher conducts a second read through the transcripts (and other data collected through participant observation, document analysis and so on) and begins initial or open coding procedures. In this step, one assigns ‘descriptors’ or ‘codes’ to text segments or passages. A code is typically a researcher-generated construct that assigns meaning to the data passage and sets the stage for category construction.8 24 Some researchers recommend a line-by-line coding technique that involves labelling or assigning codes to each line of the written data.25 Grounded theorists advocate the use of gerunds or verbs that act as nouns (ending in ‘ing’) to signal action and process, as qualitative research generally involves the study of a process over time. When applicable, in vivo codes are assigned. In vivo codes are verbatim phrases taken from the participants to capture the meaning of the line or text passage. Coding is recursive; the researcher will repeat this step several times, each time rereading passages and reworking the codes. The coding process allows the researcher to get closer to the data and provides new insights that help facilitate fine tuning of the codes. During this process, the researcher begins to foreshadow what will ultimately become categories. In the Minority Health Disparities Study, we developed an Excel matrix for each interview question and the codes for each interviewee’s response. Using this matrix enabled us to see the responses and codes for each question, which helped us to recognise patterns and categories as they emerged from the data. Table 4 illustrates how we organised the analysis showing three responses to question 10 of our semistructured interview protocol and two of the multiple rounds of collaborative coding that were undertaken.
Example of an Excel coding document used in the Minority Health Disparities Study*
Although we used hand-coding and an Excel matrix in the Minority Health Disparities Study, there are several computer software programs available designed for qualitative data analysis that many prefer over hand-coding techniques. There are detailed discussions in the literature documenting the advantages and disadvantages of using computer programs in data analysis, decision-making guidelines as to whether or not to use them, and available options and features of currently available software programs.7 8 19 In this case, we opted to develop our own hand-coding procedures we found successful as a research team and, given the small sample size (13), we implemented these as outlined here.
Step 4
Generating categories and assigning codes to them constitutes the process of constructing categories by looking for similarities among the codes, narrowing or ‘winnowing’ the codes to eliminate overlap and redundancy, and focusing specifically on codes that address the research questions. In this manner, the researcher condenses the initial broad range of codes (often well over 100) into fewer more manageable and relevant units. This process of grouping open or initial codes into categories is often called axial coding, analytical coding or focused coding.8 This is an interpretive process that extends open coding by looking for patterns that represent recurring elements in the data. A category is ‘a type or grouping of similar or closely related codes or concepts generated through inductive data analysis’.26 Names of the categories are derived from the researcher, the participant in the form of in vivo codes or the research literature. These categories should be consistent with the goals of the research, exhaustive, mutually exclusive and reflective of the data.8 In the Minority Health Disparities Study, we grouped our initial codes into categories following the procedures outlined above and subsequently organised them into themes.
Step 5
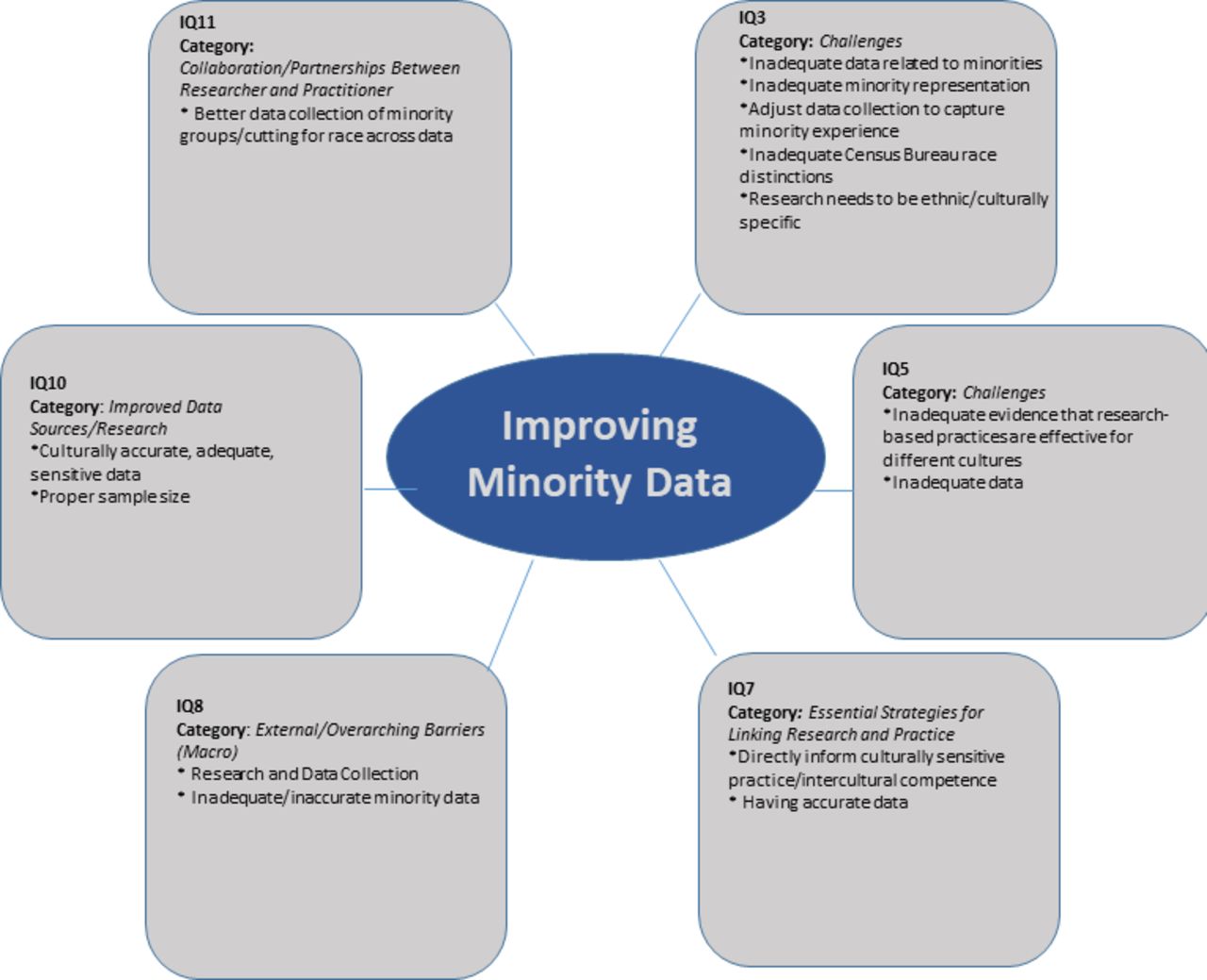
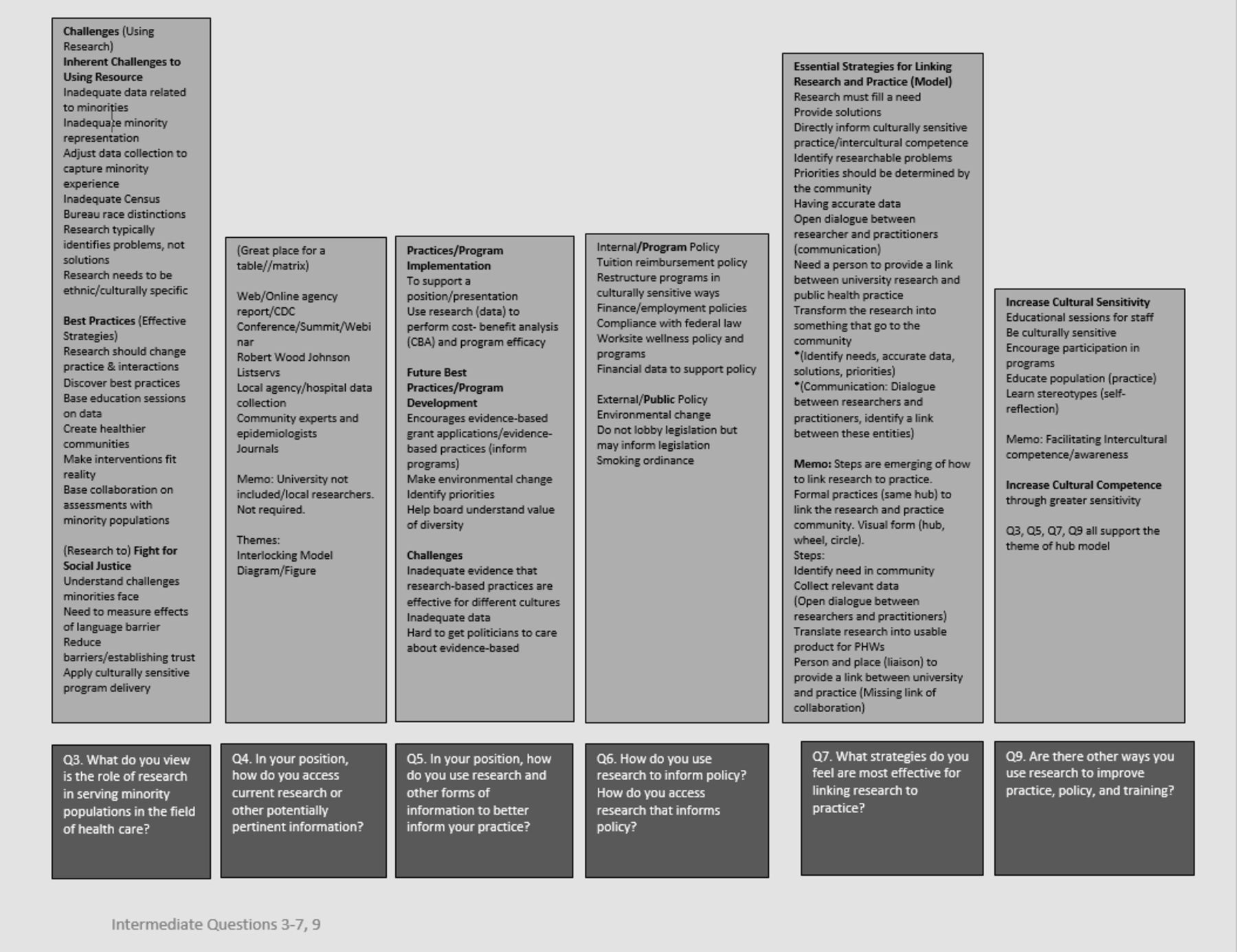
Although categories in and of themselves can and often do represent the findings of a qualitative study, qualitative data analysis involves generating themes from categories, a process by which the researcher compares categories and looks for the story they tell. This gets at the very heart of the study as the researcher looks for overarching themes that cross-cut the data and categories. Some researchers use the terms categories and themes as synonyms, but I prefer a three-step coding process from codes to categories to themes that we used in the Minority Health Disparities Study. One initially develops as many as 25–30 categories7 8 that can be subsequently reduced to fewer (10–12) categories and/or 5 or 6 themes. Figure 1 provides a visual depiction of several of our emerging categories in the Minority Health Disparities Study. Figure 2 is a visual display of one of our five emergent themes (improving minority data). Other themes included fighting for social justice, priority setting and applicability of the research, collaboration, and research accessibility.
Step 6
Strategies of validation is a process employed throughout multiple phases of the research. In their seminal work Naturalistic Inquiry, Lincoln and Guba 27 recast qualitative research criteria under the umbrella term of trustworthiness and coined new terms to describe a host of rigorous qualitative procedures that run parallel to those used in quantitative designs.27 Other scholars built on this work outlining types of validity procedures and evaluative criteria for qualitative research.28–30 Although it is beyond the scope of this paper to elaborate on these, the three common strategies used in our minority health disparities research to strengthen the credibility of our findings were (1) member checking, where the findings in the data analysis phase were sent to participants for review; (2) peer review, sharing our work with colleagues for their input; and (3) multiple coders, where two of the researchers independently coded data and then worked collaboratively to refine categories and themes.
Step 7
In qualitative research, findings are written in a narrative format to bring the reader into the setting to give them a sense of ‘being there’, thereby offering an intimate portrayal of the central phenomenon being studied. Building off member checking, peer review, memoing and ongoing data analysis, interpreting and reporting findings from participants was used to weave quotes into the discussion of findings, a common and requisite strategy in qualitative research. Table 5 provides an example of quotes that represented the theme ‘Priority Setting and Applicability of Research’ from the Minority Health Disparities Study.
Quotes from participants for theme 3: priority setting and applicability of research in the Minority Health Disparities Study*
Step 8
In step 8, interpreting and reporting findings from the literature, we developed a table of quotes/passages from the literature that supported the themes for write-up (table 6). In qualitative research, situating one’s findings in the context of the broader literature is particularly critical for bolstering the discussion of these findings. Unlike direct quotes used in the write-up of the findings, quotes from the literature were used for reference purposes and are generally not presented as direct quotes in the ensuing narrative.
Quotes from the research literature that support the theme priority setting and applicability of research in the Minority Health Disparities Study
Step 9
Visual representation of data and findings underscores the importance of visually representing qualitative data and findings through tables, figures, graphs and diagrams (see figures 1 and 2) for an example from the Minority Health Disparities Study). Visual displays are important for all types of research but take on increased status in qualitative and mixed-method research to visually enhance the narratives presented.

Visual depiction of emerging categories during data analysis for participant responses to interview questions 3–9 in the Minority Health Disparities Study.
{kind=link}
{kind=link}
Visual display of theme 2 ‘Improving Minority data’ from the Minority Health Disparities Study.
Step 10
In the strengths, limitations, delimitations and suggestions for future research, the researcher then outlines contributions to the literature of the research project and discusses challenges faced in the process. As qualitative research demands ‘transparency’ in terms of the investigator’s positioning and in the conduct of the research, this step further elaborates the details of the study. Strengths of the Minority Health Disparities Study centred on participants’ perspectives elucidating how to improve links between research and practice in the area of minority healthcare at the local, regional and national levels to better tie educational institutions of higher learning into local communities’ efforts to improve healthcare for traditionally underserved groups. Limitations included a small sample size made up exclusively of administrators and an over-reliance on one primary form of data collection (interviews). Future research called for increasingly more emphasis on community-based participatory approaches involving more sites, individuals and institutions in the research.
Conclusion
Arguably the most challenging aspect of qualitative research is data analysis, requiring training and practice for researchers to learn and devise a workable system and hone their skills. It is important to reiterate that there are no mutually agreed on guidelines for conducting qualitative data analysis, but there are overlapping commonalities among the different approaches identified above. Researchers new to qualitative research should begin by reading one or more of the chapters cited here by Creswell and associates,7 18 19 21 Marshall and Rossman,22 and Merriam and Tisdell.8 Detailed supplements to these sources are Miles, Huberman and Saldana’s Qualitative Data Analysis: A Methods Sourcebook 31 and Saldana’s Coding Manual for Qualitative Researchers,24 both comprehensive works on coding and data analysis. Another informative text is Charmaz’s Constructing Grounded Theory, a must-read for qualitative researchers.25 Flick’s The Sage Handbook of Qualitative Data Analysis 32 and Gibb’s Analyzing Qualitative Data are other useful resources.33 While methods texts are instrumental for building foundational knowledge of qualitative data analysis in the field of family medicine, the best strategy to master this skill is through practice and experimentation to learn which approach works best for you.
Acknowledgments
I would like to give special thanks to Dr Lesa L Brand and Dr. Tiffany T. Young, Department of Teaching, Learning, and Teacher Education, University of Nebraska-Lincoln, for their helpful comments and suggestions on this manuscript. In addition, I would like to thank the reviewers and the coeditors of this volume for their insightful feedback in the preparation of this manuscript.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.