Article Text

Abstract
Refugees are at increased risk for developing mental health concerns due to high rates of trauma exposure and postmigration stressors. Moreover, barriers to accessing mental health services result in ongoing suffering within this population. Integrated care—which combines primary healthcare and mental healthcare into one cohesive, collaborative setting—may improve refugees’ access to comprehensive physical and mental health services to ultimately better support this uniquely vulnerable population. Although integrated care models can increase access to care by colocating multidisciplinary services, establishing an effective integrated care model brings unique logistic (eg, managing office space, delineating roles between multiple providers, establishing open communication practices between specialty roles) and financial (eg, coordinating across department-specific billing procedures) challenges. We therefore describe the model of integrated primary and mental healthcare used in the International Family Medicine Clinic at the University of Virginia, which includes family medicine providers, behavioural health specialists and psychiatrists. Further, based on our 20-year history of providing these integrated services to refugees within an academic medical centre, we offer potential solutions for addressing common challenges (eg, granting specialty providers necessary privileges to access visit notes entered by other specialty providers, creating a culture where communication between providers is the norm, establishing a standard that all providers ought to be CC’ed on most visit notes). We hope that our model and the lessons we have learned along the way can help other institutions that are interested in developing similar integrated care systems to support refugees’ mental and physical health.
- Delivery of Health Care, Integrated
- Mental Health Services
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Refugees are persons who have fled their country due to war, political or social conflicts, mass violence, forced displacement, loss of property and community, persecution, and/or exposure to human rights violations.1 As many as 50% of refugees are expected to experience prolonged adverse mental health symptoms following resettlement,2 although estimates vary widely.3 Common mental health concerns in this population include post-traumatic stress disorder (PTSD), adjustment disorders, major depressive disorder, anxiety disorders, somatoform disorder and substance use disorder.4
High rates of mental illness among refugees can be explained by two compounding sources of distress: premigration traumas and postmigration stressors.3 Exposure to multiple forms of trauma—including persecution, life-threatening situations, and physical and sexual violence—prior to and during migration—increase risk of mental illness.5 6 Following resettlement, the stresses of adapting to a new culture,7 8 facing discrimination, xenophobia and racism,9 and navigating a charged sociopolitical environment10 in the new host country all further tax the mental health of refugees. These stressors may be especially deleterious given that community cohesion, social capital and other protective factors are often disrupted by the circumstances around forced resettlement.11 Some studies have even found that postmigration stressors are more devastating to mental health outcomes than premigration traumas.12–14 Further compounding refugees’ risk is their low access to mental health services in their new host countries, causing ongoing suffering within this vulnerable population.15 16
Integrated care reduces barriers to mental health services
Integrated care, which combines primary healthcare and mental healthcare into one cohesive, collaborative setting,17 has emerged as an effective way to address the unmet mental health needs of the general population within the USA.18 Integrated care may be especially critical in promoting early access to mental healthcare services for refugees,3 because stigma around mental illness and/or lack of cultural norms to pursue mental healthcare (given infrastructure strains within the home country having likely impeded the development of such norms) might deter some refugees from seeking independent mental health treatment.19 By colocating mental health services within primary care, refugees who present to their physician with psychosomatic or other mental health concerns can be seamlessly offered mental health interventions—from behavioural health and/or psychiatry specialists—without the need to identify, travel to and establish care at an independent mental health clinic. Such independent mental health clinics may have only limited culturally responsive care options, while primary care settings which specialise in treating refugees attract and train providers who strive to practice with cultural competence and humility.4 Beyond reducing barriers, ongoing integrated care also offers multiple opportunities to identify and intervene regarding refugees’ mental health concerns beyond those identified during the initial domestic medical examination’s mental health screen.19 20 Abu Suhaiban et al’s review found that integrated care models for the refugee population are not commonly implemented at present. This is especially concerning given that early detection and treatment of mental health disorders shortens their course and limits their impact21 22 and wait time to receive clinical services has been robustly associated with higher rates of mental health symptoms among refugees.19 This finding suggests a need to improve integrated care services for this uniquely vulnerable population.3 19 We examined our current model of integrated care at the University of Virginia Health System to investigate its reach.
International Family Medicine Clinic at the University of Virginia
The International Family Medicine Clinic (IFMC), as described by Elmore et al, is an integrated care team composed of attending physicians, nurse practitioners and second-year and third-year family medicine resident physicians with dedicated clinic time for seeing refugees; a clinical pharmacist; a registered nurse care coordinator and social worker dedicated to the IFMC refugee population; two attending clinical psychologists and doctoral students in clinical psychology; and an attending psychiatry physician and fourth-year psychiatry resident physicians who participate in the Global Mental Health Track. The IFMC provides comprehensive, culturally sensitive care to the growing refugee, asylee and immigrant populations in Central Virginia. Language interpretation is provided in person or via a remote interpretation service by trained interpreters, unless the patient notes that they would prefer their visit to take place in English. Since its inception in 2000, over 4000 patients from 87 countries have been served by the IFMC. The present paper provides greater detail regarding the integrated mental healthcare services provided within the IFMC. First, we describe the family medicine, behavioural health and psychiatry teams and the integrated mental health services they provide in table 1. Then, we describe the various pathways towards mental healthcare that are supported by our integrated care system. Finally, to characterise the patient population served, we describe who has been referred to mental health services following an IFMC primary care visit throughout the past 5 years. We conclude by briefly describing the challenges we faced when establishing the IFMC to support transparency for other health systems looking to strategically build a similar model of care.
Description of integrated care team
Pathways to mental health services within the IFMC
If a patient wishes to schedule their own appointment with psychiatry or our behavioural health team, which is hereafter referred to as the Family Stress Clinic (FSC), they may call Family Medicine’s front desk at any time to request an appointment. For patients who are non-English speaking, they can leave their name and preferred language and a front desk team member will return their call with an interpreter.
During primary care visits, the patient can benefit from the integrated care model without necessarily being brought into contact with a mental health provider through a provider-to-provider consult. Such consultations allow the primary care physician to seek insight or recommendations directly from an FSC or Psychiatry team member in advance of or during the primary care visit. Mental health specialists are always available by pager for such consultations and, during certain clinic hours, an FSC team member is available for in-the-moment consultation in the resident precepting room. Warm handoffs, by contrast, allow FSC providers to join the patient’s primary care visit, introduce themselves and the services they provide, and either provide targeted interventions on the spot (eg, initiate a behavioural health appointment) or schedule a separate follow-up appointment for targeted intervention, depending on the patient’s preference and availability. Warm handoffs are preferred over referrals to behavioural health because patients who receive a warm handoff are much more likely to schedule and attend a subsequent visit for behavioural health services than patients who simply receive a referral.18 However, when a warm handoff is not feasible, primary care physicians can also place referrals to FSC and psychiatry following the patient’s primary care visit.
FSC and psychiatry can also dynamically refer between their two clinics as treatment needs unfold. Other team members that facilitate these referrals include our social worker and registered nurse care coordinator (eg, by helping coordinate transportation, by helping the patient build trust in the clinic, by answering patient questions about insurance; see reference 23 for a full description of all specialty members comprising the IFMC).
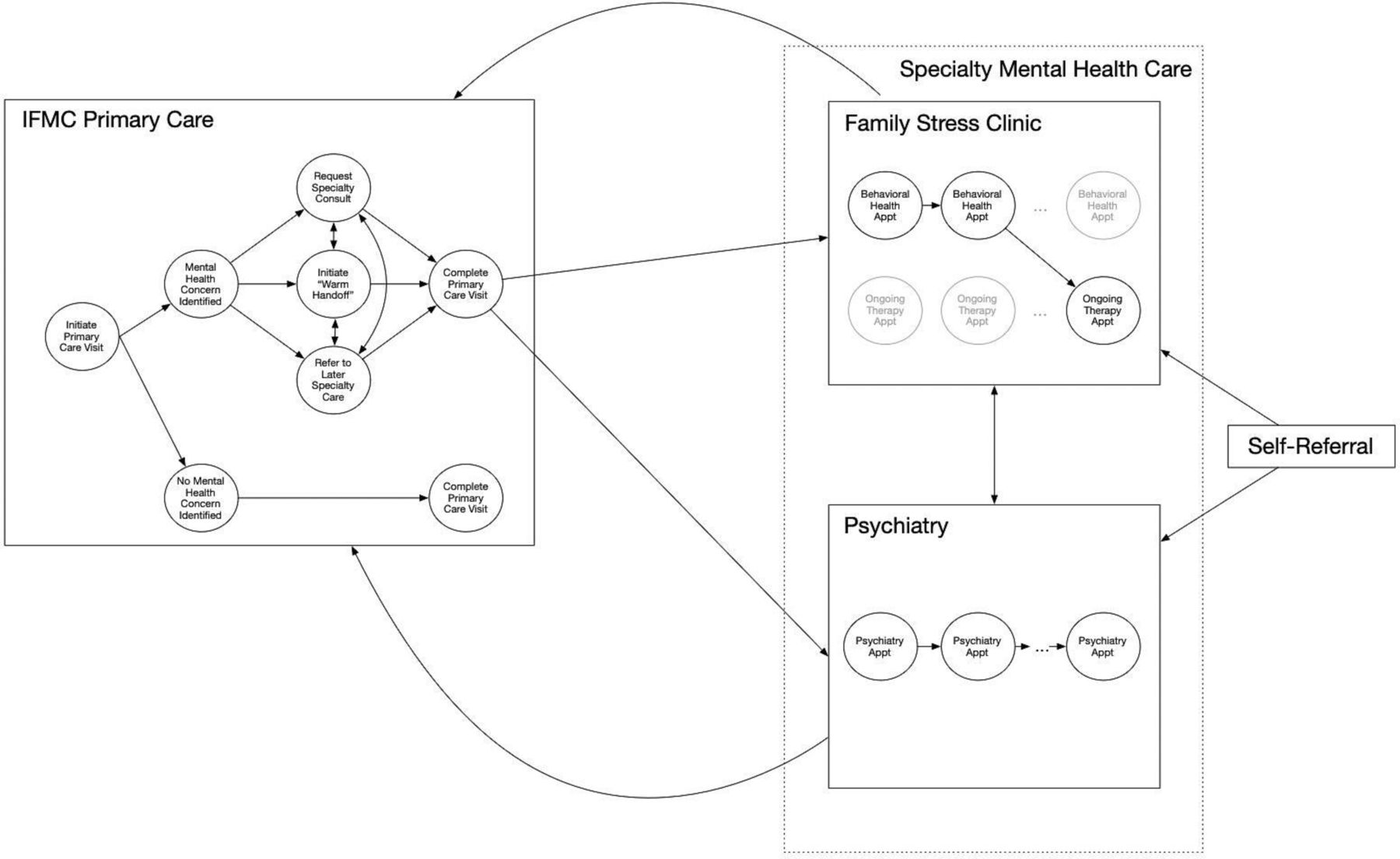
Taken together, IFMC patients can access mental health services through self-scheduling, provider-to-provider consultations during primary care visits, warm handoffs during primary care visits or referrals to follow-up care. See figure 1 for a visual representation of these referral pathways.

{kind=link}
Depiction of referral pathways. Referrals occur dynamically between and within care teams. Family Stress Clinic (FSC) box illustrates how FSC patients can transition from engaging in behavioural health appointments to engaging in ongoing therapy appointments, although this transition need not occur. For example, some FSC patients initially start with ongoing therapy before transitioning to behavioural health appointments. Others use only behavioural health or ongoing therapyservices. Appt, Appointment; IFMC, International Family Medicine Clinic.
IFMC patients served via referral to mental health services
To characterise the IFMC patients who recently went on to access mental health services within our integrated care clinic, we first identified all patients who had a mental health diagnosis listed as their primary diagnosis from a primary care provider (family medicine MD or NP) visit between 1 January 2016 and 31 December 2021. Out of the 966 patients seen in the IFMC during this time frame, 111 (11.5%) had a primary mental health diagnosis identified during their visit. The most common mental health diagnosis listed in the primary care providers’ notes was depression (49.5%), followed by anxiety (27%), and mixed anxiety/depression (6.3%). Of the 111 patients identified, 82 (73.87%) went on to attend at least one appointment with either FSC or psychiatry, suggesting that our integrated care model helped redirect at least 8.5% of our refugee patients to specialised mental health services during a 5-year span. See box 1 for three case studies that illustrate various referral pathways that refugee patients attending a primary care visit with a chief mental health complaint might take after subsequently being redirected to mental health services.
Case studies
Jita, a young adult refugee from a South Asian Country
Jita presented to her IFMC initial visit reporting a complex medical history, significant trauma history, depressed and anxious mood, restricted eating and low body weight. During her IFMC visit, Jita’s provider paged FSC and a doctoral student then joined the end of the visit, introduced themselves and FSC’s services, and scheduled an initial behavioural health appointment with Jita for the next day. Jita completed two behavioural health appointments, which focused on helping her establish care with the Teen and Young Adult Health Centre for eating disorder management, before transitioning to ongoing psychotherapy at FSC. Weekly FSC sessions focused on safety management, identity formation, processing traumatic experiences and reducing anxiety and depressive symptoms. Jita’s FSC therapist also engaged in care coordination with the Teen and Young Adult Centre, the International Rescue Committee, Jita’s high school counsellors and her primary care team. After 6 months of treatment with FSC, Jita decided to establish care with psychiatry for medication management alongside continued psychotherapy with FSC.
Deeba, an adult refugee from a Middle Eastern Country
Deeba presented to FSC for a behavioural health appointment at the request of her cousin. Her cousin was concerned about Deeba’s anxiety and health in the context of Deeba’s eldest daughter not yet being able to escape Afghanistan. Deeba reported significant physical symptoms (eg, tingling in her hands, headaches, muscle aches). She also described low energy, tearfulness, difficulty eating and trouble connecting with her younger children. Deeba completed three behavioural health appointments, which provided supportive therapy and helped Deeba identify coping strategies that brought her relief (eg, prayer, playing with her younger children, diaphragmatic breathing). Deeba also informed her FSC provider that she was confused about the various medications that had been prescribed to her, which allowed the FSC provider to help Deeba communicate this confusion to her primary care team and ultimately feel more confident in her physical health treatment. Deeba then decided to establish care with psychiatry for antidepressant medication management throughout her high-risk pregnancy.
Rayan, a teenage refugee from a Southwest Asian Country
Rayan endorsed suicidal ideation when completing a depression symptom screener during an IFMC visit. His primary care provider consulted FSC, who then joined the visit to complete a risk assessment and develop a safety plan with Rayan. FSC was reconsulted a few weeks later when Rayan reported at a follow-up IFMC visit that his suicidal ideation had increased in intensity and frequency. FSC again engaged Rayan and Rayan’s mother in safety planning and helped initiate a bed search for inpatient treatment. Following inpatient treatment, Rayan established care with psychiatry for antidepressant medication management and psychotherapy.
Identifying information has been changed to protect patient confidentiality.
Patients who followed up with our mental health services tended to be somewhat younger (M=37.28 years old) than patients who declined to do so (M=41.97 years old), which is consistent with previous work showing that older adults are less likely to perceive a need to seek mental health help than younger adults.24 However, this difference in age between those who did and did not follow up with a mental health provider was not statistically significant (t=−1.18, p=0.256). Further, men tended to be more likely to follow up with our mental health services compared with women (80% vs 71.6%, respectively, although this difference was not statistically significant, χ2=0.42, p=0.515). Although this pattern runs counter to US trends,25 it may be that lack of childcare more frequently acts as a barrier to women in our patient population. That said, we try to reduce this barrier by inviting parents to bring their children into visits, as needed, which often happens. See online supplemental table S1 for additional diagnostic and demographic information regarding IFMC patients who received a primary mental health diagnosis at their primary care visit.
Supplemental material
Of the 82 patients who followed up with a mental health provider, it was most common to do so only with FSC (46.34%), whereas 15.85% were seen only by psychiatry and 37.80% were seen by both FSC and psychiatry. Diagnoses per the mental health visit tended to more often account for the trauma-related and stressor-related nature of the mental health concern’s origin compared with those given by the primary care provider: Whereas only one patient was given a PTSD diagnosis by their primary care provider, close to two-thirds (63.41%) of the patients who followed up with FSC and/or psychiatry were subsequently diagnosed with either adjustment disorder or PTSD. These follow-up diagnoses may have offered patients greater self-understanding and validation, along with opportunities for more tailored treatment (eg, cognitive processing therapy, prolonged exposure). Other common diagnoses following a mental health visit included major depression and anxiety disorders.
Patients diagnosed with a trauma-related or stressor-related disorder during their mental health visit were more often seen by FSC or FSC/psychiatry (80.77%) than psychiatry alone (19.23%). No additional patterns in the relative likelihood for any diagnosis to be seen by FSC versus psychiatry emerged, suggesting that patient preference might guide referral pathways. For example, patients who were only seen by psychiatry tended to be older, on average (M=44.69 years old), than patients who were seen by FSC (M=35.42 years old for patients seen by FSC alone and M=36.45 years old for patients seen by both FSC and psychiatry, although neither of these differences were statistically significant, ps>0.087). See online supplemental table S2 for additional descriptive information regarding those who followed up with mental health treatment, including the average number of visits attended per patient.
Considerations for establishing a refugee-centred integrated model of care
Here, we describe challenges—and their potential solutions—that may arise when establishing a refugee-centred integrated care model, based on our 20-year history of providing these integrated services within an academic medical centre. These can be organised into logistical and financial challenges.
Logistical challenges included identifying the physical space for visits to occur (ie, whereas FSC was already colocated within family medicine’s primary care clinic, psychiatry was housed separately within the larger hospital system), determining the scope of patients served (ie, how to respond to referrals that are placed for immigrants who are not refugees or asylees), and clearly defining the roles and responsibilities between prescribing family medicine and psychiatry providers (ie, patients sometimes ask their family medicine provider to refill a prescription that was initially written by their psychiatrist; the psychiatrist might wish to stop a medication that was prescribed by the family medicine provider). We managed these challenges by reserving an office within family medicine’s primary care clinic for psychiatry visits to take place in 1 day per week, limiting services to refugees and special immigrant visa holders and improving communication procedures between primary care, psychiatry and FSC (ie, creating a culture where communication between providers is the norm and is expected, establishing a standard that all providers ought to be CC’ed on most visit notes, and by providing family medicine and FSC providers access to psychiatry visit notes, which had initially been protected), respectively.
Financial challenges included determining which department would bill for IFMC psychiatry visits that occurred in family medicine office space and how to fund the cost of language interpretation services. Unlike FSC, which is housed in the department of family medicine, the department of psychiatry is distinct at the University of Virginia Health System. As such, the first billing challenge is unique to psychiatry visits. We managed the psychiatry billing challenge by advocating for the following agreement: IFMC patients seen for primary care and FSC visits are billed for those services through their insurance by the department of family medicine. IFMC patients seen for psychiatry visits, even though those visits take place within family medicine offices, are billed for those services through their insurance by the department of psychiatry. No finances are exchanged between the psychiatry and family medicine departments and patients are not billed separately by the department of family medicine for facility fees during psychiatry visits. Most patients have Medicaid insurance, which covers these visits. However, in some necessary cases, providers may offer their time pro bono. With respect to the cost of language interpretation services, under Title VI of the Civil Rights Act of 1964 and Executive Order 13166, people with limited English proficiency are required to be provided with meaningful access to language interpretation services at no cost to them from agencies that receive federal funding. Hospitals that receive Medicaid and/or Medicare insurance payments are, therefore, obligated to provide interpretation services at no cost to patients. The cost of trained language interpreters within our healthcare system is covered by the medical centre at large rather than by individual departments. As such, no cost for language interpretation is incurred at the department-specific level.
While idiosyncratic challenges may arise within any given centre, and unexpected challenges can arise over time (eg, due to policy changes, due to centre-specific or hospital-wide administration changes or staffing shortages, due to new culturally responsive training needs as the patient population shifts), we hope to communicate that these challenges can be managed, especially by interested, passionate and skillful providers who step up to be champions of this work within each of the specialty roles. In our experience, appreciation of and recognition for the roles taken on by such invested champions grows over time and ultimately becomes embedded within the clinic’s care culture, which itself helps to stimulate continued interest and investment in these roles.
Conclusion
Refugees are at increased risk for developing mental illness due to high rates of trauma exposure and postmigration stressors.3 We describe an integrated care model that has reduced barriers to accessing mental health services for refugees. Between 1 January 2016 and 31 December 2021, at least 82 new IFMC patients from 12 countries speaking 14 languages established care with behavioural health, psychiatry or combined behavioural health/psychiatry services following a referral from their primary care provider. Over this time frame, 872 unique visits in psychiatry and FSC were delivered. This self-study emphasises the demand for mental health services by refugees who have recently resettled in Central Virginia and describes a model that can be used by other centres. Future research is needed to evaluate refugees’ outcomes within this integrated model of care.
Ethics statements
Patient consent for publication
Ethics approval
The use of audit data from this review of records was approved by the University of Virginia’s Institutional Review Board for Health Sciences Research #23852.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @KatharineEDani2
Contributors KED led manuscript writing and data analysis. SRB collected data from EMR and provided edits to manuscript. JST, RLM, FRH and CA all lead different areas of patient care within the described integrated care model, were secondary writers on the manuscript and edited the manuscript.
Funding This study was funded by Jefferson Scholars Foundation (John S. Lillard Fellow), Philanthropic Educational Organization (Scholar Award).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.